|
Dandy-Walker
malformation is a cystic dilatation of the fourth ventricle or a cyst in
communication with the 4th ventricle, with a varying degree of vermian
agenesis, often associated with hydrocephalus.
The
Dandy walker malformation was initially described in 1914 by Dandy and
Blackfan, who described a case of an enlarged fourth ventricle which was
presumed to result from a fourth ventricle outlet obstruction. In 1954, the term Dandy Walker malformation
was introduced by Brenda.
Pathogenesis
The
exact pathogenesis of Dandy walker syndrome has since been the subject of
continuous debate. The syndrome probably represents a nonspecific
central nervous system malformation, which may occur alone or with other
malformations and which may occur in single gene disorders, in
chromosomal aberrations, or as a consequence of an environmental insult.
The cause of Dandy-Walker syndrome is unknown. Despite the common
association of other congenital anomalies with this syndrome (including
other central nervous system, cardiac, gastrointestinal, urogenital,
facial, and skeletal anomalies), this condition has been only occasionally
described in families, most often as part of a syndrome inherited in an
autosomal recessive manner. This
syndrome may also occur in the context of chromosomal aberrations. Other
associated nervous system abnormalities may include agenesis of the corpus
callosum, aqueductal stenosis, cerebral heterotopias, holoprosencephaly,
neural tube defects, and rachischisis. Before 1984, with 300 reported
cases of Dandy-Walker syndrome in the literature, only 16 had been
described in families, suggesting that a genetic predisposition to this
syndrome probably is uncommon.
The
syndrome probably represents a nonspecific central nervous system
malformation, which may occur alone or with other malformations and which
may occur in single gene disorders, in chromosomal aberrations, or as a
consequence of an environmental insult. Four theories have been proposed
for this developmental abnormality.
Dandy
and Blackfan and later Taggart and Walker f were of the opinion
that congenital occlusion of the foramina of Luschka and Magendie was the
principal factor responsible for the dilatation of the 4th ventricle and
the secondary maldevelopment of the cerebellar vermis. The reasons
proposed for the absence or presence of hydrocephalus included an abnormally
small choroid plexus producing less quantities of fourth ventricular
fluid, the cyst wall acting as a semipermeable barrier resulting in the
escape of fluid from the cyst into the subarachnoid spaces, and
absorption of the cyst fluid by vessels lying in the cyst wall. Gibson13
however showed that the outlet foramina of the fourth ventricle could be
patent.
Benda
believed that the malformation was principally a failure of fusion of the
corpus cerebelli.
Others
believed that a neuroschistic cleft and bleb at the region of the corpus
cerebelli, without rupture of the ectoderm, resulted in adhesions with
the inner dural layer and inhibited the development of the vermis. This
meant that imperforation of the roof of the fourth ventricle was not the
cause of the anomaly but only a part of it.
Gardner12 felt that
delayed permeability of the fourth ventricle roof causes a foetal
hydrocephalus. This, together with an earlier developed posterior choroid
plexus causes excessive distending forces in the posterior fossa leading
to a dilated fourth ventrticle, a large posterior fossa, and a high
placed tentorium. Gardner also described a variant of the malformation,
'the Dandy-Walker cyst' In this anomaly ventricular
fluid accumulates between two layers of the ependyma to form a true
cyst.
Pathology
The
cystic fourth ventricle has a wall separate from the dura of the
posterior fossa. The outer layer of this wall is arachnoid and the inner
layer ependyma. A layer of tissue derived from the-cerebellum lies between
the two layers. This middle layer becomes more apparent laterally and
superiorly. The outlet foramina of the fourth ventricle are patent in
43-82 per cent of the cases reported in the literature.
The
choroid plexus of the fourth ventricle is hypoplastic and is displaced
caudally and lies near the brainstemornearthedilated lateral recesses.
The degree of involvement of the inferior vermis is variable. Even when
it seems that the vermis is entirely replaced by the cyst wall,
hypoplastic vermian tissue may be seen on microscopy. The
superior vermis is often displaced superiorly, The cerebellar
hemispheres are displaced laterally and dorsally and show the effects of
hypoplasia and secondary atrophy due to chronic pressure. The brainstem
is flattened antero-posteriorly. Hydrocephalus is usually present with
dilatation of the lateral and third ventricles. The cause of the
hydrocephalus may be aqueduct stenosdis, fourth ventricular outlet obstruction
to the CSF path ways.
Clinical
Features
Dandy-Walker
malformation accounts for about four per cent of all cases of
hydrocephalus10.
The
clinical features depend on the effects produced by the cyst, the
presence or absence of hydrocephalus and associated anomalies.
62
per cent of patients with the malformation present during the first year
of life, 17 per cent between the first ana fifth years and 11 per cent
during the second decade of life.
Infants
present with symptoms and signs of raised intracranial pressure,
including vomiting, a bulging fontanelle and sixth nerve paresis. The
occipital region is usually prominent, the shape of the skull tending
towards dolichocephaly. Transillumination of the posteriorfossa in
infants is positive and will also allow differentiation between the
malformation and a posterior fossa extra-axial arachnoid cyst.
Children
over two years of age present with headache and papiiloedema. Ataxia is
present in more than 50% of the patients and
delayed milestones and mental retardation is seen in upto 40 per cent of
these children.
Seizures, motor deficits, cerebellar signs other than
ataxiaand brainstem signs may also occur. Often there may be only a
macrocephaiy. Sutural diastasis is commonly found. The lambdoid suture
may be found split mere than the others, occasionally to such an extent
that the occipital bone is found "floating".
Investigations
The Dandy-Walker malformation develops at approximately 4
weeks gestation. After the first trimester, ultrasound is useful in
identifying the cyst and other brain anomalies.
MRI is the choice of imaging. Principal features on MRI
include partial or complete agenesis of vermian, dilatation of the 4th
ventricle, enlarged posterior fossa with elevation of the tentorium, and
cerebellar hypoplasia. In mega cisterna magna, the 4th ventricle is
normal with no vermian hypoplasia. The 4th ventricle is displaced in
arachnoid cysts.
MR provides a detailed anatomic study of the structures in
the posterior fossa and also of all the associated anomalies
present. Barkovich
et a have, on the basis of MR studies of
posterior fossa cysts and cyst-like malformations, proposed a new
classification in which the Dandy-Walker malformation, the variant and
the mega cisterna, magna, form part of a continuum of a single
developmental anomaly which they called the ''Dandy-Walker complex".
The Dandy Walker variant is a less severe malformation. the vermis is
hypoplastic, but not absent, and the posterior fossa is not enlarged.
Joubert's syndrome is characterized clinically by ataxia,
mental retardation, episodic hyperpnoea, and abnormal eye movements, and
is due to total aplasia of the cerebellar vermis. On CT or MR1 where, in
addition to absence of the vermis. the fourth ventricle appears large and
triangular with the apex pointing backward at its mid portion. and large
and 'bat's wing' at a higher level.
The absence of the vallecula suggests a Dandy-Walker
malformation while a normal vallecula and a compressed fourth ventricle
suggest an arachnoid cyst. The "key-hole sign" is seen with a
cyst which is isolated from the ventricular system.
The differential diagnosis of a posterior fossa include, arachnoid cysts, Dandy-Walker malformation,
and mega cisterna magna.
|
|
|

|
|
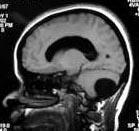
Post.
fossa arch. cyst- MRI
|
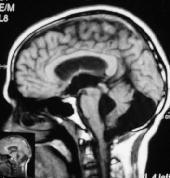
Dandy-walker
cyst-MRI
|
Mega
cisterna magna-MRI
|
|
An arachnoid cyst results in anterior
displacement of the fourth ventricle, but normal cerebellar development.
|
Dandy-Walker malformation is a cystic dilatation of
the fourth ventricle or a cyst in communication with 4th ventricle.
|
Mega cisterna magna is an anatomic
variant with normal fourth ventricle and small cerebellum.
|
CT-ventriculography using water soluble contrast material is
perhaps the best for preoperative assessment of the ventricular system
and the CSF pathways. This not only provides information on the patency
of the aqueduct but will also clearly rule out a posterior fossa arachnoid
cyst.
Treatment
20%of the cysts are asymptomatic and require no
intervention. Treatment is controversial.
Direct fourth ventriculostomy, as advocated by Dandy, was
the treatment followed till the advent of shunting devices. Shunting
procedures are the treatment of choice for the Dandy-Walker malformation.
In the presence of hydrocephalus, there is no question that a ventricular
shunt has to be inserted. What is under debate, however, is the need for
shunting the posterior fossa fluid collection. Ventriculoperitoneal
shunt may allow the cyst grow larger and herniated upward. Excising the
cyst has been tried virtually with no success. Combined shunting of the
supra and infra tentorial compartments is probably the optimal treatment.
However, many others feel that this double shunting is not
necessary as a primary procedure. Ventriculo peritoneal shunt may
allow the cyst grow larger and herniated upward. Excising the cyst has
been tried virtually with no success. Combined shunting of the supra and
infra tentorial compartments is probably the optimal treatment. The
double shunt may be inserted, if necessary, in two stages. In the absence
of hydrocephalus, a cysto-peritoneal shunt may be performed.
The results of the shunting procedures have been uniformly
satisfactory. Adults and older children have a better prognosis as they
tend to have fewer associated abnormalities than infants. The presence of
associated anomalies did not correlate with low IQ scores except in those
pateints with agenesis of the corpus callosum. The control of
hydrocephalus is one of the more important factors in determining the
intellectual development of these patients. Approximately, 50% of long
term survivors have an IQ of 80 or more and approximately 30% have normal
intelligence.
|
