|
In Japan, germ
cell tumors constitute 2% to 9% of all intracranial tumors, with a male
preponderance. The incidence is less in the west and other countries.
Germ cell tumors are thought to arise from primitive cell nests found
along the embryonic midline.
They include,
germinoma, mature, immature, and malignant teratoma, choriocarcinoma,
endodermal sinus tumor, embryonal cell carcinoma, and tumors of combined
histology.
Two thirds of all
are germinomas. Teratomas are the next commonest.
Teratomas and
choriocarcinomas occur more commonly in childhood. Most other tumors are
diagnosed during second decade of life, raising the possibility of an
associated neuroendocrine changes taking place during puberty.
Overall, germ cell
tumors of the CNS most commonly arise in the pineal and suprasellar
regions, pineal site being more common in boys than in girls. Germinomas
occur equally in suprasellar and pineal regions. Germ cell tumors
account for more than half of all pineal region tumors. Others germ cells tumors are more commonly
found in the suprasellar region. Other sites include, sacrococcygeum,
retroperitoneum, nasopharynx. They are much less frequent. There are
occasional reports of involvement of chiasma, thalamus, cerebellum, and
septum pellucidum.
Germ cell tumors
have a propensity to disseminate, either via CSF pathways or by
infiltration of contiguous structures in the range of 10% to 22%. The
rate is high (40%) in choriocarcinomas, and endodermal sinus tumors.
|
Clinically they present with symptoms associated with those of
suprasellar or pineal regions. Pineal tumors present with features of
hydrocephalus. Upward gaze paresis (Parinaud's syndrome) is
characteristic. Brain stem dysfunctions can occur.
Suprasellar
lesions tend to cause diabetes insipidus, cvisual disturbances,and
pituitary dysfunctions.
CT typically reveals a hyoperdense, enhancing midline mass.
It is
hypo to isodense on T1 and hyperdense on T2 MRI images.
Intense
enhancement with gadolinium is noted.
Cytic and
calcified components are seen.
Germinomas
are more homogenous, whereas teratomas are heterogenous.
|
|

|
|
Pineal Germinoma-CT
|
|
Pure germinomas account
for 65% to 72% of all intracranial germ cell tumors. Germinomas are
poorly circumscribed and often seed the ventricular system. They may
infiltrate the surroundings. The germinoma usually presents dark
lobulated surface and grows to a large size, so that its precise site of
origin, often remains unclear.
|
The histological picture is
distinctive, the tumor being composed of two well defined cell
types. These are groups of large polygonal of spherical cells with
large central nucleolated nuclei, separated by groups of much
smaller lymphocyte like cells with small shotty nuclei. The
latter are often distributed along the vascular connective tissue
stroma of the tumor. The larger cells do not show the
argyrophilic and other characteristics of glial cells
and may contain mitotic figures.
In a proportion of germinomas,
other tissue elements, indicative of their teratomatous nature, may
also be encountered. These include foci of glandular tissue,
cuboidal or columnar epithelium, mucus secreting cells, smooth muscle
fibers, and even squamous epithelium or cartilage. Furthermore,
the tumor may exhibit a hyperplastic neuroglial reaction, or a granulomatous
reaction including multinucleate giant cells.
|
|
|
|
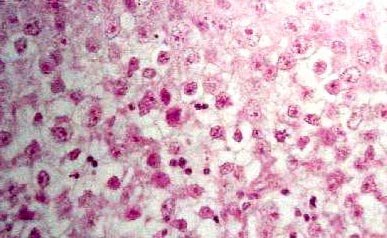
Germinoma (H&E): Groups of
large polygonal of spherical cells with large central nucleolated
nuclei, separated by groups of much smaller lymphocyte like
cells.
|
|
The relationship between embryonal carcinoma,
teratocarcinoma, endodermal sinus tumor and yolk sac tumor, though close,
is ill-defined.
Embryonal
carcinoma is the
most primitive of these tumors, and the least frequently reported
intracranial germ cell tumor. It is a primitive neoplasm composed of
pluripotential epithelial cells. This tumor rarely found in its
pure form, is usually highly malignant and is composed of sheets of
cuboidal to columnar cells with large vesicular nuclei and distinct
nucleoli.
Endodermal
sinus tumors are rare and usually highly invasive,
and characterized by a reticular network of cuboidal epithelium,
occasionally arranged in papillary patterns. Schiller-Duval bodies
characterized by delicate blood vessels surrounded by primitive columnar
cells lying in a space lined by flattened cells, are seen. Globular
intra and extracellular eosinophilic masses positive for
alpha-fetoprotein are also seen.
Chorion
carcinoma occurring in isolation in the
pineal-diencephalic region is exceptional. Areas of
syncytiotrophoblastic differentiation are found more commonly in
embryonal carcinomas, endodermal sinus tumors and germinomas than in
chorion carcinomas. The tumor is characterized by large round
cytotrophoblastic cells with clear cytoplasm alongside sheets of multinucleated
syncytiotrophoblast cells, associated with prominent blood-filled
sinuses.
Grossly, they are granular, reddish brown mass, almost
always with hemorrhage and necrosis. As all other tumors of germ-cell
origin, choriocarcinoma is usually accompanied by elements of other
tumors of this group.
Teratoma are either
immature or mature, the former resembling embryonic or fetal tissues and
the latter resembling mature or adult tissue. By definition, the term
teratoma can be used only in cases where tumor elements derive from two
or three germ layers. These tumors are usually well-circumscribed,
round or lobulated, and multicystic, and compress the surrounding
structures. The cystic component may be watery, mucoid or
sebaceous. Sometimes bone, cartilage, hair or teeth is
present. Immature tumours are more frequently associated with a
malignant course.
Microscopically,
combinations of tissue elements from the various germ cell layers are
seen in varying proportions.
|
Immunohistochemistry reveals the
intra and extracellular hyaline droplets, which contain alpha
fetoprotein (AFP) and alpha1- antitrypsin.
CSF levels of AFP and human
chorionic gonadotropin (HCG) are useful for monitoring therapeutic responses.
Their use for the purpose of
differentiation between individual germ cell tumors is unreliable.
Endodermal sinus tumors and
embryonal carcinomas are
|
|
Tumor
markers for Germ cell Tumors:
|
|
Histology
|
beta HCG
|
AFP
|
PLAP
|
|
Germinoma
|
-
|
-
|
+
|
|
Teratoma-immature
|
low
|
low
|
-
|
|
Teratoma-malignant
|
low
|
-
|
-
|
|
Embryonal cell ca
|
+
|
+
|
-
|
|
Endodermal sinus tumor
|
-
|
+
|
-
|
|
Choriocarcinoma
|
+
|
-
|
-
|
|
|
Low Beta
HCG: (<50IU/L) Low AFP:
(<25ng/mL)
|
|
positive for ‘cytokeratin’ and for
‘epithelial membrane antigen’.
PLAP (placental Alkaline Phosphatase),
beta-hCG (SCT cells) are specific for germinomas.
AFP is positive in glandular components
of teratomas.
Pineal cell tumor markers include
melatonin and the S antigen.
Currently, the recommended treatment include,
surgery, followed by appropriate chemo and radiotherapy.
A preoperative
staging with neuroaxis imaging and CSF analysis, when possible is
recommended.
Germinomas, are highly radiosensitive
and carry the best prognosis, with 5 year survival rates in the
range of 85%, and 10 years rate of 65%.
It has been suggested that teratomas,
excised completely, do not require any further treatment.
Survival for other germ cell tumors is
much less optimistic.
|
