|
The craniofacial
approach has gradually evolved over the past five decades into a safe and
reliable technique for resecting both benign and malignant tumors involving
the anterior cranial base. It can be extended and incorporated as a part
of a more complex resection involving the infratemporal fossa and
anterolateral cranial base, as well as the middle cranial fossa,
cavernous sinus etc.
INDICATIONS:
The tumors most commonly requiring combined anterior
craniofacial surgery usually begin in the nose or sinuses. Many of these
tumors to a greater or lesser degree are malignant . Inverting papilloma
is an example of transitional type of tumor that is locally invasive,
does not metastasize, but must be resected aggressively to avoid
recurrence. Esthesioneuroblastoma varies from a very indolent to a highly
aggressive tumors. Most tumors of nasal or para nasal sinus origin are
squamous cell or adenocarcinomas of the maxillary or ethmoid sinuses.
Tumors with a primary intracranial origin such as
meningioma, chordoma or chondrosarcoma require combined resection when
they clearly violate the anterior fossa floor.
SURGICAL TECHNIQUE:
General anesthesia should be performed by a team experienced
in neurosurgical procedures. A lumbar drain is routinely placed and
patients are given prophylactic per operative antibiotic. The patient is
then placed in a Mayfield head holder and positioned to optimize both the
neurosurgical and facial approaches. The leg is propped to obtain a skin
graft and fascia lata if needed.
The anterior craniofacial approach incorporates a
combination of transfacial and transcranial procedures. The facial
approach consists of a graduated greater exposure depending on the extent
of disease. The basic is done through a lateral rhinotomy approach
coupled with a low craniotomy. The lateral rhinotomy incision may be
extended into a Web-Ferguson incision if a more extensive maxillary
excision is required.
Craniotomy:
The craniotomy is tailored according to the extent of
involvement of the anterior fossa floor, the sub cranial tumor location,
and the degree of dural or frontal lobe invasion. A bicoronal scalp
incision is made running 2 to 3 cms behind the hairline. The flap is
elevated in the subgaleal plane down to the eyebrows , then to the
lateral orbital walls laterally and just below the nasal globella
medially. A large flap of pericranial tissue is created that will be used
for later reconstruction. As the dissection proceeds the brows, the
supratrochlear and supraorbital neurovascular bundles are exposed and
preserved.
The anterior cranial fossa is then exposed by removing a
segment of bone which may be pedicled on the temporalis muscle or completely
separated. The lower horizontal bone cut should be kept low to lessen the
need for subsequent brain retraction. Withdrawing 25 to 50 ml of CSF from
the lumbar subarachnoid catheter, lowering Pco2 through controlled
hyperventilation, and occasionally administering mannitol or steroids
further reduce the need for mechanical frontal lobe retraction.
The dura is then carefully dissected off the cristagalli and
cribriform plate dividing the dural sleeves that extend along the
olfactory nerves. The intracranial portion of the tumor extension is then
assessed. If it involves the dura or in certain situations, frontal lobe
this will have to be resected, together with the tumor, If the dura is
intact, it is retracted back to the planum sphenoidale.
Once the head and neck surgeon has completed the exposure
and mobilization of the tumor transfacially a chisel or drill is used
either from above or below to make the necessary bone cuts to encompass
the tumor and deliver the specimen.
|

|

|
|
bicoronal
&lateral rhinotomy incision& its extensions
|
lateral
rhinotomy
|
|

|
|
|
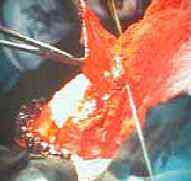
defect after
tumor removal
|
repair with
vascularized pericranial flap
|
Facial Approach:
The facial approach depends on the extent of the tumor.
Often utilizes modifications of a lateral rhinotomy incision which may or
may not transect the upper lip. This depends on whether a total
maxillectomy is done in conjunction with the resection.
The periosteum is elevated from the nasal bone as well as
from the medial and inferior surfaces of the orbit.
The nasolacrimal duct is identified and transected distally.
The anterior and posterior ethmoidal arteries are then identified and
cauterized or clipped.
In most cases it is necessary to perform a complete enbloc
ethmoidectomy. For this purpose a contra lateral lynch incision is made
to elevate the contra lateral periorbita, cauterize the anterior and
posterior ethmoidal vessels, and make the appropriate osteotomies.
If preoperative imaging studies confirm the presence of
tumor in this, the soft tissues of the orbit, then orbital exenteration
may be facilitated by extending the incision laterally to include a
portion of the eyelids.
RECONSTRUCTION:
The secret of avoidance of post operative complications in
anterior skull base surgery is the insurance of a water tight dural
closure. If a portion of the dura has been excised, it is repaired with
fascia lata.
The pericranium is used for anterior cranial fossa
reconstruction. It is usually pedicled on the supraorbital and
supratrochlear arteries. The pericranial flap is placed across the defect
in anterior cranial fossa. The distal end is clamped between the cranial
floor bone and the overlying dura. It may be secured with sutures through
the bone or anchored with fibrin glue. Unless a large amount of anterior
cranial fossa bone has been resected and concern for brain herination
exists, it is usually not necessary to place a bone graft across the bony
defect. Also, it is usually not necessary to place a skin graft on the
under surface of pericranium(facing the nasal cavity), since this tissue
has been shown to "mucosalize" readily on its nasal cavity.
Once the pericranial flap is in place the spinal drain is
clamped so that no further intraoperative CSF decompression will take
place. This will allow gradual reexpansion of the brain to make contact
with the pericranial flap, obliterating any residual dead space.
Since the pericranial flap traverses the frontal
sinus, it is necessary to obliterate the frontal sinus with fat or free
muscle after removing all the mucosa in the sinus. If the sinus is quite
large, it may be advisable to remove the posterior wall of the sinus
completely and allow the brain and dura to expand and fill the space (
Cranialization of the frontal sinus)
The bifrontal craniotomy bone flap is then replaced and
secured according to the surgeon's preference. This may be done with
wires, plates or sutures.
In all cases, an exclusive nasal pack is placed for at
least 5 days post operatively and a lumbar drain kept for the same
duration. In significantly larger defects, particularly if orbital
exenteration and facial skin is excised, a bulky free flap is considered.
Basal Sub frontal approach:
It is in many ways similar to the anterior craniofacial
resection operation except that the Transfacial exposure is less
extensive. Because the target area for this approach is more posterior
(Sphenoid and clivus) than in the anterior cranio facial resection
(ethmoid and cribriform), the craniotomy bone flap is larger, and the
orbital bone cuts are broader. This approach also begins with a bicoronal
incision.
After exposing the orbital rims, periorbita is elevated from
beneath the orbital roofs and medial walls in preparation for osteotomy.
Bifrontal craniotomy is then performed, and dura is elevated from above
the orbital roofs and cribriform areas. Using malleable retractors to
protect the brain and orbital contents, the reciprocating saw is used to
create osteotomies that result in temporary removal of both orbital roofs
and the supra orbital contents, the reciprocating saw is used to create
osteotomies that result in temporary removal of both orbital roofs and
the supra orbital bar.
The coronal osteotomies along the posterior orbital roof
should be made as far posteriorly as possible to simplify reconstruction,
by conserving orbital contour, and to prevent postoperative pulsatile
exophthalmoses.
The neurosurgeon completes the approach by drilling a small amount
of bone remaining posteriorly to unroof the optic nerves, superior
orbital fissures and sphenoid sinus. Extirpation then proceeds as
required by the tumor, followed by reconstruction which is similar to
that done for anterior craniofacial resection.
|
