|
Management of
tumors of the temporal bone and base of skull is one of the most
challenging problems. The intimate association of these tumors with
the carotid artery, jugular vein and the V through XII cranial nerves
have in the past rendered many patients inoperable.
The development of the infratemporal fossa approach, as
pioneered by Fisch, has allowed the excision of
lateral skull base and petrous apex lesions which were previously deemed unresectable.
These approaches are classified as type Fisch
A, B and C.
TYPE A approach:
This approach is used for removal of tumors involving the
jugular foramen and vertical, segment of petrous internal carotid artery,
primarily class C and D glomus temporal tumors. This approach is
also indicated for meningiomas, cholesteatoma
involving the internal carotid artery and petrous apex, for intratemporal neuromas of cranial nerves IX-XII
and for lesions reaching the skull base from below (Carotid artery
aneurysms, glomus vagale tumors etc).
Operative technique:
Surgical highlights:
Retroauriculo – cervico – temporal skin incision
Blind sac closure of external auditory canal
Facial nerve exposed in parotid
Great vessels and cranial nerves exposed in the neck
Subtotal petrosectomy
Permanent anterior transposition of facial nerve
Ligation of the sigmoid sinus
Eustachian tube obliterated
Mandible displaced anteriorly
Internal carotid artery exposed
Jugular foramen and infralabyrinthine
space exposed for tumor removal
Middle ear cleft obliterated with fat and temporal is muscle
flap.
The key point of this approach is the anterior transposition
of the facial nerve, which provides optimal control of the infralabyrinthine and jugular foramen regions, as
well as the vertical portion of the internal carotid artery.
|
A standard, curvilinear post auricular incision is
extended into the upper neck.
The anterior flap is elevated superficial to periosteium over the mastoid and deep to platysma
in the neck. The external canal is transected at the bony cartilaginous
junction and the flap continued forward over the parotid for 2-3 cms. The lateral external ear canal skin is
undermined from underlying soft tissues, everted, and over sewn to
create a blind-sac closure of the EAC. The facial nerve is dissected
out in the parotid.
The upper neck is next dissected, vessel loops are placed
proximally around the internal and external carotids and silk ties are
placed, but not yet tied, around the internal jugular vein.
The vagus and accessory nerves
are identified as they exit the jugular foramen and the hypoglossal is
noted as it crosses the carotid bifurcation.
The sternomastoid muscle is
dissected from the lateral and medial mastoid tip and mobilized with
the post auricular flap.
A well beveled canal wall down mastoidectomy
is next performed.
The remaining EAC skin, tympanic membrane, malleus and
incus are excised, and the sigmoid sinus is completely skeletonised.
The entire middle ear and mastoid course of the facial
nerve is identified using cochlear form process, horizontal
semicircular canal and digastric ridge as landmarks.
The facial nerve is decompressed to 270 of its
circumference where possible, from the geniculate ganglion to the stylomastoid foramen.
The mastoid tip and the bony EAC are quickly removed with
large cutting burr and bone roungeurs while
constantly keeping facial nerve in view.
If there is limited intradural
extension, the dura is opened without injury to the endolymphatic
sac.
Tumor is carefully removed from the carotid artery
anteriorly, if necessary. Often, a surgical plane between the
carotid artery adventia and tumor can be
identified. When such a plane is not present and tumor is
adherent to the adventitia, residual tumor is left on carotid and later
cauterized.
Deep infralabyrinthine tumor
extension may
involve
the inferior internal auditory canal, thereby placing the cranial
nerves VII and VIII at risk. At times labyrinthectomy
may be necessary to permit exposure and safe tumor removal from the
IAC.
Whenever possible, the medial wall of the jugular bulb is
left intact, thereby protecting the cranial nerves IX through
XI.
The eustachian tube is
obliterated with muscle and facial plugs.
The surgical cavity is obliterated with abdominal
fat.
The procedure described above is used for glomus jugulare tumors.
TYPE B approach:
|
|

|
|
Skin incision and blind closure of EAM
|
|

|
|
Rerouted 7th nerve
|
|
|
|
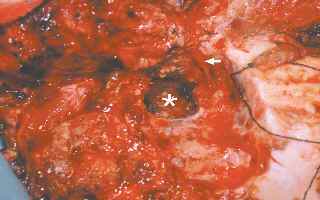
Tumor bed after excision
|
|
|
|
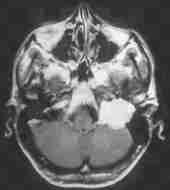
Pre and post OP CT
|
|
In this approach, the skin incision is extended anteriorly,
the zygomatic arch is divided and the petrous carotid artery is
skeletonized. The temperomandibular join
is then disarticulated, the eustachian tube
detached anteriorly with associated soft tissue, and the middle meningeal
artery and mandibular nerve divided as needed. This
provides access to the clivus and
petrous apex and is applicable to glomus tumors involving the horizontal
petrous carotid artery, clival chordoma, and congenital cholesteatoma of the petrous
apex.
TYPE C approach:
This is an anterior extension of type B and allows for
exposure of the parasellar region, nasopharynx,
pterygomaxillary fossa and eustachian
tube. It has been used primarily for extensive juvenile
nasopharyngeal angiofibroma and radiation
failure squamous cell carcinoma.
The management of intracranial tumor extension depends on
the size and location of the tumor, and the status of the patient.
Small intracranial tumor extension are removed with the jugular bulb
because this is typically the site of dural
penetration. The decision to remove large intracranial extensions
is based on the hemodynamic status of the patient.
Blood loss in excess of 3 liters usually prompts a second
stage approach to total tumor removal.
Post-operative care:
All patients who have undergone infratemporal fossa
dissection are monitored overnight in the intensive care unit for
evidence of hemorrhage or evolving neurological injury.
Postoperative hemorrhage is extremely rare
due to the extensive measures taken to ensure intraoperative vascular
control. However, given the complexities of modern skull base
surgery and the advanced stage in which most skull base tumors present, postoperative
cranial nerve deficits are inevitable. Jacksons reported that
76% of his patients with extensive skull base neoplasms suffered a new
intraoperative cranial nerve deficit, the most common being a glosso pharyngeal / vagal lesion. Likewise, Spector
found that 19% of glomus jugulare patient
suffered a partial or complete VII nerve paralysis postoperatively.
In the later stages of growth, many skull base neoplasms tend to envelop
rather than infiltrate the contiguous cranial nerves. Consequently, it
may be possible to maintain anatomic neural integrity by microsurgical
tumor dissection of the nerves, if the involved nerves are not
intentionally sacrificed during tumor removal. Because such dissection
tends to devascularize the nerve, many patients
will suffer a transient cranial nerve palsy as a result of their surgery
and will require temporary supportive care.
In all cases of facial paralysis, either transient or
permanent, it is essential that adequate corneal protection be provided
by medication, temporary taping, placement of
gold weights or tarsorrhaphy.
Because of the high incidence of transient dysphagia and
aspiration, most patients remain intubated for at least 24 hours or until
they are fully cognizant. In selected cases, tracheotomy and
nasogastric tube feeding may be required for several weeks, particularly
if multiple cranial nerve palsies including X, XI, XII have
occurred. Early vocal cord medialization, either by endoscopic teflon injection or external thyropalsty,
may be necessary to permit decannulation in
those cases with new vagal lesion and severe aspiration. In rare
instances, combined vagal and hypoglossal injury may lead to permanent
tracheotomy and gastrostomy. Except in those cases with extensive intracrianl extension, cerebrospinal fluid leak
and meningitis are rare due to the multiple layers of protection
offered by EAC and eustachian tube closure
along with mastoid cavity obliteration. When CSF leak does occur as
heralded by external wound leakage or rhinorrhea, initial treatment is
bed rest with head elevated, lumbar drainage, and pressure
dressings. If conservative measures fail wound exploration with
possible repacking of the cavity and/or ventriculo
peritoneal shunting may be necessary.
Summary:
The infratemporal fossa approach, in conjunction with the
application of microsurgical technique and improved perioperative care,
has permitted significant advances in lateral skull base surgery.
The glomus jugular tumor is the prototypical neoplasm resected by this
approach, although this technique can be applied to a host of additional
benign and malignant lesions of the skull base. This approach
entails identification and control of the cranial nerves and great
vessels in the neck, anterior transposition of the facial nerve, and infralabyrinthine petrosectomy.
Intracranial tumor extension and petrous carotid artery involvement
remain limiting factors. Significant morbidity, particularly neurological
deficit and hemorrhage, may occur due to the nature and location of
lateral skull base tumors. Recent advances in preoperative
embolization and temporary carotid artery balloon occlusion have advanced
the limits of resection via the infratemporal fossa approach.
|