|
The modern era of neurotologic transtemporal
skull base surgery began in 1961 when William House introduced the
operating microscope and multidisciplinary surgery for the removal of
acoustic neuromas with low mortality rate and enhanced facial nerve
preservation rate. An array of neurotologic
procedures provide safe exposure of the mid brain,clivus, CPA, petrous apex and infratemporal
fossa.
The
objective of transtemporal surgery is obtaining
wide skull base exposure by precise dissection of the temporal
bone. These collaborative techniques by neurotologist
and neurosurgeon provide wide surgical exposure and minimize brain
retraction. Knowing theanatomy of the temporal
bone is essential to understand about these approaches.
Anatomy of Temporal Bone:
The
temporal bone contains and is surrounded by many important
structures. It articulates with five other
cranial bones: the frontal, parietal, sphenoid, occipital and
zygomatic.
It can be divided into four parts: the squamous,mastoid, petrous and tympanic.
a) Squamous portion:
The
lateral surface defines the boundary of the middle cranial fossa.
It extends medially to join the superior surface of the petrous bone in
the region of the tegmen.
b) Mastoid portion:
Pneumatization within the mastoid process
is variable. The squama of the temporal bone forms the lateral wall
of the central air containing space, the antrum, which communicates with
middle ear by the aditus. The suprameatal spine and cribrifom
area provide important landmarks for surgical access to the anturm. From here pneumatization
may extend inferiorly into the tip of the mastoid process. Pneumatization also extends into the perilabyrinthine region and petrous portion of the
temporal bone.
c) Petrous portion:
The
petrous portion of thetemporal bone roughly
assumes the configuration of a four-sided pyramid. Within the body
of the petrous bone is found the labyrinth and internal carotid artery,
CN VII and CN VIII, all penetrate the bone substance. The medial
wall of the middle ear cavity contains the first turn of the cochlea.
d) Tympanic portion:
The
tympanic part of the temporal bone forms the anterior and inferior walls
and part of the posterior wall of the external auditory meatus.It is separated anteriorly from the squamous
bone by the tympanosquamous suture more
medially from the petrous bone by the petrotympanic
fissure and posteriorly from the mastoid portion of the petrous bone by
the tympanomastoid fissure. The
inner part of the tympanic
ring is grooved and is called the tympanic sulcus, which accomodates the tympanic membrane
annulus. The inferior aspect of the tympanic bone is
elongated into a vaginal process immediately anterior to the styloid
process.
Superior and anterior surface:
This
forms part of the middle cranial fossa. The foramen lacerum is found between the apex of the petrous bone
and sphenoid bone and contains but does not transmit the ICA. Near
the apex is a small depression which lodges the trigeminal
ganglion. The arcuate eminence of the petrous bone overlies the
superior semi-circular canal. The tegmen
tympani is lateral to the eminence. The opening of the hiatus of
the facial canal is anterior and medial to the arcuate eminence; this
transmits the superficial petrosal branch of the middle meningeal artery
and the greater petrosal nerve.
Posterior cerebellar surface:
Posterior
surface of the petrous bone forms the anterolateral surface of the
posterior fossa. A sulcus for the superior petrosal sinus defines
its superior border.Posteriorly it articulates
with the occipital bone.
Approximately midway between the apex and the anterior border of sigmoid
sulcus is the IAM. It is a short canal begins medially at the
internal acoustic pore.A bony plate which is
also part of the medial wall of the cochlea and vestibule closes the
lateral end. A horizontal ridge of bone, the transverse crest,divides thepore into upper and lower areas. Theanterior portion of the superior division contains
the facial nerve which is separated from the superior vestibular nerve in the posterior portion of the upper
division by a small, vertical crest of bone,known
as ' Bill's bar'. It serves as an important landmark during the translabyrinthine approach. The cochlear
nerve lies in the anterior portion and the inferior vestibular
nerve in the posterior
portion of the lower
division. Midway between the meatus and sigmoid sulcus, is the
vestibular aqueduct which transmits the endolymphatic sac and duct.
Inferior surface:
Most
irregular of the petrous bone'ssurfaces. The
opening of the carotid canal is aboutmidway
between the apex and base; this is the entrance for the ICA and its plexus of veins and sympathetic nerves.
The canal courses in a cephalad direction along the anterior wall of the
tympanic cavity to the bony eustachian
tube and then bends horizontally,ending at the
apex of the petrous bone and the occipital bone. Carotid ridge is a
sharp bone separating the carotid and
jugular foramen. The lateral part of the foramen contains the
sigmoid portion of the transverse sinus; the medial part contains the
inferior petrosal sinus and the glossophayrngeal ,vagus and accessory nerve.
Anterior to the lateral compartment is the broad fossa for the jugular bulb. Posterior and lateral to
it is the styloid process. Lateral
to its base is the stylomastoid foramen
transmitting
facial nerve.
Facial nerve:
The
facial nerve lies in the anterosuperior part of
IAM, anterior to Bill's bar. It
passes laterally over the labyrinth (Labyrinthine segment) to reach the geniculate ganglion.There
it makes as acute bend, running posteriorly upto
the lateral semicircular canal (tympanic segment). There it takes
90 degree bend to run in the inferior
direction (mastoid segment) before it exits through the stylomastoid foramen.
Surgical approaches:
Approaches that traverse the otic capsule (Transcapsular) permit wide exposure but sacrifice
hearing: translabyrinthine (TL), Trans otic (TO) and Transcochlear
(TC).
Posterior
approaches that spare the otic
capsule (Retro capsular) provide varying degrees of CPA exposure with an
opportunity for hearing preservation: retro labyrinthine (RL), retro
sigmoid (RS).
Superior
approaches (Supra Capsular) permit unroofing
of the internal auditory canal (IAC) with varying degrees of petrous apex
exposure and an opportunity for hearing preservation: middle fossa (MF)
and extended middle fossa (EMF).
The inferior
approaches: infracochlear (IC) and infralabyrinthine (IL).Removal of the otic capsule provides the most direct
route to the IAC and CPA without the need for brain retraction.
1) TRANSLABYRINTHINE APPROACH:
The TL approach is applicable for CPA and IAC lesions of all sizes
especially in patients with poor hearing. Even though this approach
is popularized for acoustic neuromas, it is suited for any neoplasm requiring exposure of the CPA.
In patients without useful hearing, the TL approach is also useful for
facial nerve tumours and vestibular neurectomy.
|
Technique:
Surgical Highlights
· Retro auricular incision
· Cortical Mastoidectomy
· Posterior labyrinthectomy
· Exposure of the
internal auditory canal
· Identification of the Facial nerve at the meatal foramen
|
|
|
|
. Removal of lesion or nerve section
· Aditus, mastoid cavity and vestibule
obliterated with musculo facial graft and
fat.
|
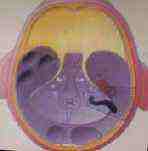
|
extent of bone
removal in translab.approach
|
|
The
patient is supine with the head turned to the opposite side.
A
curved post auricular incision is made with the apex 3 to 4 cm
posterior to the post auricular crease.
Complete
cortical mastoidectomy is performed.
The
tegmen and posterior
fossa dural plate are identified and
the sigmoid sinus is skeletonized.
Exposure
of the retrosigmoid posterior fossa dura for
at least 1 cm behind the sigmoid sinus is important.
Anteriorly
the facial nerve is identified in its vertical segment but left covered
with bone
for protection against inadvertent
burr trauma.
|
|

|
|
Next step is labyrinthectomy by drilling out the semicircular
canals. Care is taken to leave the anterior wall of
the lateral canal, and the most anterior part of the
ampulla of the
superior canal in
order to protect the tympanic and labyrinthine portions of the
facial
|
|
lateral, posterior
& superior semicircular canals seen after cortical mastoidectomy
|
|
nerve and to serve as a
landmark for the superior vestibular
nerve.
All
IAC bone removal is completed before the dura is opened and the IAC neural structures are exposed.
IAC
skeletonization begins by drilling a trough
along the inferior edge of the vestibule until the jugular bulb is identified - the inferior limit of
dissection.
The
anterior limit of dissection is the cochlear aqueduct. Once the
inferior border of the IAC is identified, a superior trough is drilled
along the superior edge of IAC. A full
of 270 degree skeletonization of the IAC dura is critical to prevent
bony edges from interfering with adequate tumor removal.
Particular attention is required along the lateral extent of
|
|

|
|
the
IAC to preserve crucial landmarks for facial nerve dissection
|
|
labyrinthectomy in progress
|
|
Tumor Removal:
In small lesions the tumor is exposed by opening the dura
of IAC. The superior vestibular
nerve is transected by placing an angled instrument adjacent to Bill's
bar and reflecting the superior vestibular nerve and it identifies the lateral plane between the facial nerve
and the tumor. Sharp and blunt dissection can proceed without
actually placing traction on the facial nerve.
|
|

|
|
In large tumors, CPA exposure is necessary. Intracapsular tumour debulking is completed
before
the tumor is dissected directly from the facial nerve. After
tumor removal eustachian tube is packed with surgicel
and temporalis muscle.
|
|
bone surrounding the IAM removed for 270
degrees. Tumor in the IAM seen
|
|
The dural defect is loosely approximated
with sutures and the mastoidectomy defect is filled
with strips of abdominal fat.
The TL approach provides wide and direct access to CPA
tumors with minimal cerebellar retraction.
It permits identification of the facial nerve - laterally
at the fundus and medially at the brain stem, which helps in anatomic
preservation of the facial nerve.
|
|
|
|
The disadvantage
of this approach is that hearing cannot
be preserved.
|
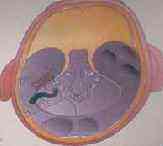
|
extent of bone removal in transcochlear approach
|
|
2) TRANSCOCHLEAR
APPROACHES:
While
TL approach offers wide exposure of the CPA,the cochlea and petrous apex block access to
the anterior aspects of the CPA and the ventral brain stem.
A spectrum of transcochlear
approaches provide access to the ventral brain stem, beginning with the
transotic (TO) and extending to a true transcochlear (TC), with the widest exposure being
the transpetrous (TP).
|
|

|
|
All these
approaches, by definition, remove the cochlea following a TL approach
to extend the exposure anteriorly.
The facial nerve remains in situ (although skeletonized)
in the TO approach,
|
|
subtotal petrosectomy done. semiocircular
canals being drilled out.;tympanic &
mastoid segment of facial nerve decompressed
|
|
The facial nerve
is transposed posteriorly in the TC approach.
The TP approach includes the full TC with the addition of
an infra temporal fossa approach and even transposition of the petrous
carotid artery in certain cases.
The disadvantage of this approach is that
hearing cannot be preserved.
3) TRANSOTIC APPROACH:
|
|

|
|
Surgical Highlights:
|
|
facial nerve exposed;exposure
of geniculate ganglion & GSPN
|
|
Retro auricula-temporal incision
.Blind closure of external auditory canal
.Subtotal petrosectomy
.Tympanic and mastoid fallopian canal left as a bridge
over the cavity
Otic
capsule removed to expose the complete medial surface of the
temporal bone.
Maximal trans temporal exposure of the internal auditory canal and
CP angle.
Direct anterior approach to the intrameatal and intracranial facial nerve.
Dura reconstructed with musculo facial graf.
|
|

|
|
Cavity obliterated
with fat and temporalis muscle flap.
Through a postauricular incision, ear is reflected
anteriorly, and the external auditory canal
|
|
posteriorly rerouted facial nerve lying
on the posterior fossa dura
|
|
is
transected and closed in two layers. The soft tissue exposure,
complete mastoidectomy, labyrinthectomy,posterior
and middle fossa dura decompression, and
skeletonization from the geniculate
ganglion to the stylomastoid foramen,
while
maintaining a thin egg shell of bone on the nerve are
carried out.
The
retrofacial air-cell tract is also dissected, permitting 360-degree skeletonization of the facial nerve in the
vertical and tympanic segments. Then the cochlea is drilled out
and the petrous carotid artery is the anterior limit of the
exposure. By working around the facial nerve, the surgeon has
access to lesions of the IAC, CPA, clivus and
jugular foramen. Closure is performed with obliteration of the defect with abdominal
fat.
|
|

|
|
|
|
cochlea
is drilled out.
|
4)
TRANS COCHLEAR APPROACH :
Like TO, the TC approach combines the TL with removal of the cochlea;
however wide access to the anterior CPA is provided by posterior
transposition of the facial nerve. Thus the exposure extends from
the sigmoid sinus posteriorly to the petrous carotidartery
anteriorly.
The
posterior transposition of the facial nerve results in an obligatory
temporary facial paralysis that produces some degree of aberrant
regeneration. The fifth,seventh,
ninth, tenth, and eleventh cranial nerves, the clivus,
both the vertebral arteries and the basilar artery are routinely
seen.
One
added advantage of the approach is that during bony dissection to obtain
exposure, the blood supply and the tumor
base are removed, which is particularly important in
petrous ridge meningiomas.
The
principle indications for this approach are large petro-clival meningiomas, epidermoids, extensive gliomas, jugular
tumors and even temporal bone
malignancies.
Technique:
Surgical Highlights:
Retro auriculo temporal incision
Blind closure of external auditory canal
Subtotal petrosectomy
Posterior labyrinthectomy
Exposure of internal auditory canal
Decompression of mastoid, tympanic and labyrinthine segments of
facial nerve and geniculate ganglion
Division of greater superficial petrosal nerve and posterior
rerouting
Drilling out of anterior wall of IAC, cochlea,petrous
tip and clivus
Removal of tumor
Cavity obliterated with fat and temporalis muscle flap
Posterior transposition of the tympanic and vertical segments of the
facial nerve requires transection of the greater superficial petrosal
nerve. Following facial nerve transposition, cochlea and tympanic
ring removal exposes the carotid artery anteriorly, the jugular bulb and
inferior petrosal sinus inferiorly and the superior petrosal sinus
superiorly.
This approach provides direct access to the base of implantation and
blood supply of tumors arising from petrous tip and petroclival
junction. Temporary facial nerve paralysis occurs uniformly with
the posterior transposition of the facial nerve which is most likely the
consequence of devascularization of the perigeniculate segments of the nerve caused by
transection of the greater superficial petrosal nerve and its
accompanying vessels.
5) TRANSPETROUS APPROACH
In this procedure, full TC exposure is combined with infratemporal fossa
approach, orbitozygotomy and even transposition
of petrous carotid artery. This approach is indicated in only the
most extreme extension of tumor into the lateral cranial base and intracranially.
|
