|
CNS
melanotic lesions include, the rare primary melanomas, and the commoner
secondary melanomatous deposits.
Occasionally
other common intracranial tumors also show melanotic pigmentations.
Classification:
Russel
&
Rubenstein (1989)'s informative classification is given below:
1) Normal meningeal pigmentation - melanocytosis
2) Neurocutaneous syndrome (Patchy meningeal pigmentation, may be
familial, no pathological sequelae)
3) Neurocutaneous melanomatosis (diffuse meningeal pigmentation,
neural infiltration, hydrocephalus, very rarely familial).
4) Primary meningeal melanocytoma (synonymous with melanotic
meningioma, pigmented meningioma, cellular blue naevus
biologically and histologically benign, local recurrence is common,
mitosis are rare, necrosis and hemorrhage are rare,
50% may be spinal often associated with cervical nerve roots).
5) Malignant meningeal melanoma (leptomeningeal tumor, may be
intra-axial or extra-axial, biologically benign or
frankly malignant, leptomeningeal seeding, may arise in any of the above
settings, diffuse multi-focal nodular pattern,
50% not associated with cutaneous nevus, 4% of these tumors may be
associated with neurofibromatosis,
nevus of Ota, Sturge Weber syndrome).
For
practical purposes, they may be classified as primary melanomas,
secondary melanomas, and melanotic tumors.
WHO(2000)
classifies primary melanomas as,
1) Diffuse Melanocytosis
2) Melanocytoma
3) Malignant melanoma
4)
Meningeal Melanomatosis
Pathology:
Primary
CNS melanomas:
Melanocytes
originate from the ectodermal cells of the neural crest by the
6th week and migrate in their destination reaching the skin by
the 10th week and the meninges by the 20th week of
embryological development. These cells produce melanin pigment contained
in melanosomes and are found in the epidermal-dermal junction, uveal
layer of the eye and importantly in the basal meninges, piamater and on
the ventral aspect of the medulla. The convexity is free.
Increased
number of melanocytes in the central nervous system in association with
congenital melanocytic naevi a phenomenon is known as Neurocutaneous
melanosis. Thick sheets of melanocytes are found in the
pia and arachnoid, most commonly over the base of the brain,
and in the parenchyma of the basal ganglia, dentate nucleus,
cerebellar hemispheres, pons, thalamus, and amygdala.
Neurological
symptoms may occur; these may be caused by abnormalities of
circulation, resorption of cerebrospinal fluid, local pressure
effects, or malignant transformation.
Melanomas
arise
from melanocytes. Primary central nervous system melanoma is a rare
disease in contrast to cutaneous melanoma which is the fastest increasing
malignancy in western populations. Diagnosis of a primary melanoma
can be made only after a thorough autopsy to exclude a primary elsewhere.
Only about 300 cases of primary cerebral and spinal melanomas have been
reported. Autopsy reports suggest cerebral metastases are found in 32% of
deaths from melanoma and and the incidence may be higher, if non
investigated strokes are included.
Tumors
arise where melanocytes are concentrated predominantly at the base of the
brain and in the upper cervical spine;
nine
cases have been described in the pineal gland. Other rare sites include
the pituitary gland and the choroids plexus. It is thought that
melanocytes reach these remote locations long pial arachnoid sleeves
associated with blood vessels.
Primary
CNS malignant melanomas occur early (30-39years), when compared
with cutaneous melanoma, (50-60 years).
Tumors
occur either as diffuse leptomeningeal proliferations
or occasionally, as a discrete mass.
Rarely,
the tumor is benign (melanocytoma), but in general they are
malignant from the onset.
Malignant
change is complex, probably the result of polygenic deletions.
The
presence of a giant cutaneous nevus (greater or equal to 50cm) is the
only reported association. These abnormal naevi have an inherent
increased risk of malignant development compared with normal naevi. The 5
year cumulative risk for neurocutaneous melanocytosis is about 2.5%.
Multiple
chromosomal alterations have been identified as the cause.
Familial
disease occurs in 4-10% of cases and is highly penetrant in an autosomal
dominant pattern, with a likely locus on chromosome1.
No
environmental factors, unlike the cutaneous variety, have been identified.
Secondary
CNS melanomas:
Cutaneous
melanoma is a highly malignant tumor with a predilection for neural
metastasis.
Melanoma
is the third most common malignancy to metastasize to the
brain after lung and breast carcinoma.
One
Australian series quotes a clinical incidence of 32% for cerebral
metastasis. Metastastic melanomas are more common than the primary.
Some
studies identify the scalp, neck and trunk as sites with a greater
predilection to cerebral metastasis. The BANS regions (Upper Back,
Posterior Arms, posterolateral Neck, posterior Scalp) are often quoted as
being worse prognostically. This probably reflects thicker lesions
at the time of late presentation.
The
brain is the initial site of metastasis in
12-20% of patients. Occasionally, patients may present with brain
metastases and an unknown primary. This phenomenon may be secondary to
spontaneous regression of a primary lesion or de novo melanoma within the
lymph nodes, gastrointestinal tract, respiratory tract, or vagina.
Approximately 10-20% of patients with an unknown primary have had a
pigmented lesion removed in the past or have noted a pigmented cutaneous
lesion that has involuted.
Leptomeningeal
involvement is common.
Melanoma
rarely presents as a cerebral metastasis at initial diagnosis, occurring
in only 2% of cases.
Frontal
and parietal lobes are affected most frequently and lesions arm commonly
subcortical in location and require advanced techniques of intraoperative
localization.
Multiple
lesions occur twice as frequently s single deposits; 16-25% of patients
have the CNS as their only site of metastasis.
Spinal
metastases constitute1% of large series and may occur at any level.
The
median interval between diagnosis of cutaneous disease ad CNS involvement
is variably 29 months, to 42 months.
Histologically, melanomas and
other melanocytic derived tumors are variable in their appearance.
They are commonly composed of spindle shaped cells with large nuclei and
prominent nucleoli. Mitosis may be scant or numerous. Necrosis and
mitoses are hallmarks of malignancy.
On
immunohistochemistry, S-100 is expressed by almost all melanomas, though
it may be variable in its intensity. However it is also positive
for schwannomas and sarcomas. HMB-45 is more specific for
melanocytic cells but may be negative in metastatic deposits. Thus
its positivity in cerebral and spinal lesions may suggest primary
disease. Melanomas do not express epithelial markers.
Clinical features:
Presentation
is usually due to increased intracranial pressure with headache being the
primary symptom in 45-50%, seizures in 15-22%, motor disturbance in 15%
or a cerebral catastrophe in 24% of cases at diagnosis.
|
Imaging:
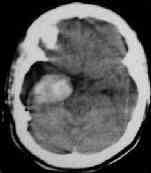
On
CT scanning the melanoma is characteristically hyperdense and
enhances uniformly; areas of cystic formation are not uncommon.
Hemorrhage and necrosis are common. Lesions are usually large at
the time of presentation, typically subcortical with associated
surrounding edema.
MR scanning
better demonstrates necrosis and intra-tumoral hemorrhage and edema
associated with malignant. MRI may show clinically silent lesions not
demonstrated on a CT scan. On T1 images, they are hyper/isodense
relative to brain. T2 signals may be variable.
|
|
|
|
Melanoma
with intratumoral bleeding
|
|
|
|
Lesions
are solitary in 25% of cases. A solitary metastasis with hemorrhage in a
young person without a known extra cerebral primary malignancy is
suggestive of melanoma.
Melanoma
is a great mimicker of other tumors. Suspicion in the presence of
suspicious looking cutaneous nevus is the key.
With
the advent of non-invasive imaging techniques, such as magnetic resonance
imaging, it has been established that patients with congenital
melanocytic naevi may be associated with a variety of non-melanocytic
anomalies of the CNS, including Dandy-Walker malformation, encephalocoele,
vermian hypoplasia, arachnoid cyst, and Chiari type I malformation.
Management:
Optimal
management remains elusive. CNS melanotic lesions may be
asymptomatic in a small group of patients. Neither the frequency nor the
natural history of asymptomatic intracranial melanosis has been
established; the incidence of asymptomatic ones is considered to be low
in long term follow-ups.
Surgery for solitary
cerebral metastases is widely accepted as the best option.
The
overall outlook remains poor, average survival with conservative measures
after neurological presentation is 2-3 months. Management of
multiple lesions remains problematic.
Untreated
cerebral disease progresses rapidly. Most studies demonstrate
improved survival rates with surgery.
2
year survival rate is about 10%.
Leptomeningeal
involvement can only be managed with adjuvant therapy.
Adjuvant
therapy includes, palliative whole
brain radiotherapy in conventional doses (30 grays/18 fractions)
against cerebral melanoma provides symptomatic relief in up to two thirds
of patients.
Stereotactic
radio surgery
may be a suitable alternative treatment for tumors of less than 3 cm
diameter as well as for debilitated patients or those with deep lesions
unsuitable as surgical candidates.
Stereotactic
radiotherapy
may be combined with whole brain palliative radiotherapy.
Steroids
are
effective in symptomatic relief but only extend survival to two months,
on average.
Most
chemotherapeutic drugs have been used against
melanoma. None has been shown to be superior in isolation or in
combination therapy. Dacarbazine (DTIC) is
the only chemotherapeutic agent approved by the US Food and Drug
Administration (FDA) for melanoma. The exact mechanism of action of DTIC
is unknown. The drug is administered intravenously at a dose of 2-4.5
mg/kg/day for 10 days. This may be repeated at 3-week intervals. Other
useful drugs include decarbazine, nitrosureas, and vinca alkaloids which
may produce partial remission in 15-30%, and complete remission in 5-10%
of cases. However remission is short-lived.
Melanoma
has provided a useful model for immunotherapy.
Interesting results have been achieved with large doses of
alpha-interferon and interleukin-2 but remission is partial and short
lived. Specific tumor infiltrating lymphocytes selected and
expanded from tumor specimens and cultures with interleukin-2 demonstrate
tumoricidal effect. Immunotherapy may offer an effective means of
eliminating small volumes of residual disease, and as such may be of
benefit to patients having undergone resection of cerebral lesions.
Prognosis:
Neurologically
symptomatic CNS melanosis is considered to carry a very high
mortality rate. Hence, it has been suggested that the children with a
congenital melanocytic naevi greater than 2 cm in
diameter on the head or over the spine, should have a careful
neurological and developmental assessment by a pediatrician at
presentation, and should continue to be followed closely
during at least the first two years.
Untreated
cerebral disease is rapidly fatal within 1 month of diagnosis.
Steroids may extend survival a further month. Whole brain radiotherapy
improves quality of life for 2-4 months before fatal remission
occurs. Average survival after surgery is better than 9 months but
few patients survive beyond 12 months. Focused radio surgery requires
further evaluation but is a good option for the patient with unresectable
disease or in poor clinical condition not suitable for craniotomy.
Immune system activation and modification may provide further windows of
opportunity for treatment of systemically active disease as well as for
minimal volume residual disease.
Other
melanotic CNS tumors:
Other
neural crest derived cell lines may also produce melanin.
Accordingly,
those tumors may also exhibit pigmentation that resembles that which is
seen in melanocyte derived tumors; they have no clinical
significance. Medulloblastoma, ependymoma, choroids plexus
papilloma, meningioma, astrocytoma, acoustic neuromas and pituitary
adenoma may appear pigmented and be melanin positive. Melanotic
schwannoma may be difficult to differentiate from primary nerve root
differentiate from primary nerve root melanoma. Differentiation between
meningeal melanomas, true melanotic meningiomas and melanotic schwannomas
is even more difficult because of common reactivity to
immunohistochemical markers.
|