|
SPONDYLO is a Greek word meaning vertebra. Spondylosis
generally mean changes in the vertebral joint characterized by increasing
degeneration of the intervertebral disc with subsequent changes in the
bones and soft tissues. Disc degeneration, spinal canal stenosis,
spondylolisthesis are the resultant pathological changes.
Disc degeneration is
the commonest pathological manifestation of lumbar spondylosis. (discussed elsewhere)
Lumbar spinal stenosis can
be defined as ‘narrowing of the lumbar canal in its central part, the
lateral recess or the intervertebral foramen sufficient to impair one or
more roots of the cauda, the impairment resulting in pain, unilateral or bilateral
neurological deficit or neurogenic intermittent claudication’. Lumbar
spinal stenosis appears in different pathological conditions. The
form that is discussed here is mainly due to degenerative disease. The
epidemiology of lumbar spinal stenosis has changed a great deal in the
last few decades, related to the ageing population of industrialized
countries, with a growing impact on national health systems.
Anatomy:
The spinal canal is formed anteriorly by the intervertebral
disc or the vertebral body, lateral by the pedicles, posterolateral by
the facet joints and posteriorly by the laminae or the yellow
ligament. The spinal canal has paired lateral openings in each
segment, the intervertebral foramina.
The lateral recess if the lateral part of the spinal
canal. It begins at the tip of the superior articular process of
the inferior vertebra, which is part of the facet joint. It is at
this point where the recess is narrowest. After bending laterally
around the pedicle it ends caudal in the broader lateral opening of the
spinal canal, the intervertebral foramen. The anterior wall of the
lateral recess is bounded by the intervertebral disc superiorly, and the
vertebral body inferiorly. The lateral walls are formed by the vertebral
pedicles. The dorsal wall is bounded by the superior articular
process of the lower vertebra, to a small part by the lamina and also by
the yellow ligament. In a narrow lateral recess, its dorsal walls
built only by the articular process, and it is the degenerative changes
of this structure that account for most of the nerve root compressions in
lumbar spinal stenosis.
The nerve roots corresponding to each segment are separated
from the dural sac at the level of the intervertebral space then they
come to lie in the lateral recesses and exit the spinal canal a level
below through the intervertebral foramina. At each of these points
compression is possible.
Pathogenesis and classification:
The term idiopathic developmental by Verbiest in 1954
as a disease of unknown origin, with a genetic disturbance in which
pathological effects are revealed in their entirely only when growth is
complete and the vertebrae have attained full size’. This
review will concentrate on the type of lumbar spinl stenosis that was
classified as idiopathic developmental stenosis by Verbiest or
considered to be degenerative lumbar spinal stenosis by other
authors. Most authors accept the theory that explains lumbar spinal
stenosis through degenerative changes that lead to instability and nerve
root compression which causes problems if the individual anatomy of the
spinal canal is unfavorable.
Developmental and congenital factors include some of the
anatomical variations that leave less space for the nerve roots, so even
minor degenerative osseous changes can lead to nerve root compression: a
shallow spinal canal, a trefoil shaped canal, or anomalies of the nerve
roots.
Anatomical variations in the orientation, shape, or
asymmetry of the facet joints make degeneration more likely that lead to
nerve root compression. Degeneration is more likely to cause symptomatic
nerve root compression in a narrow spinal canal, than in wide canal in
which even pronounced spondylosis or spondylarthrosis may stay clinically
silent.
The trefoil shape of the spinal canal is anatomical
variation of the spinal canal, caused by the orientation of the
laminae and facet joints. Most often it is found at the levels L3
to L5. This condition is considered to be a predisposing factor for
the development of lateral recess stenosis through degenerative changes
of the facet joints.
Anomalies of the nerve roots, (conjoined roots, redundant
roots, transverse roots) can also contribute to the development of
signs. A disproportion between the size of the lateral recess and
the diameter of an aberrant root is needed to develop symptoms.
Asymmetric facet joints hasten disc degeneration, frontally
oriented facet joints allow a wider range of lateral bending and
therefore also have a negative impact on disc integrity. At
the same time they leave less space in the lateral recess.
Sagittally oriented joints allow easier sagittal displacement of a
vertebra-development of degenerative spondylolisthesis. Acquired
factors include all degenerative changes that lead to osseous and
non-osseous nerve root compression.
|
Morphologically
the following forms of impingement of nervous structures occur either
alone or in combination can be differentiated in lumbar spinal stenosis:
·
Central spinal stenosis
· Lateral
recess stenosis
· Narrowing
of the intervertebral foramen
· Non-osseous
nerve root compression
|
|

|

|
|
|
spinal canal stenosis-Axial MRI
|
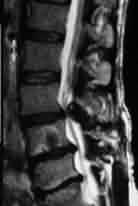
Facetal hypertrophy-MRI sagittal
|
Spinal canal stenosis-Sagittal MRI
|
|
The causes of central spinal stenosis are spondylarthrosis,
formation of spondylotic ridges, thickened lamina, or degenerative
spondylolisthesis. Spondylarthrotic facet joints can almost touch,
narrowing the posterior portion of the spinal canal. Spondylosis
with posteriorly directed oesteophytes, combined with spondylarthrosis
can cause marked narrowing of the spinal canal with little space left for
the nerve roots and an atrophy of the epidural fat. Thickening of
the lamina occurs in advanced cases of degenerative changes and plays a
minor role in reducing the diameter of the canal.
Different parameters have been used to measure the extent of
central stenosis of the spinal canal, among them measurement of the
sagittal diameters of the spinal canal and measurement of the dural tube
in square millimeters are commonly employed. The traditional
measurement of the sagittal diameter, under 10 mm being considered
pathological.
Lateral recess stenosis is the most common form of
degenerative spinal stenosis that occurs either alone or in combination
with central stenosis. Usually the compression of the nerve root is
caused by a spondylarthrotic facet joint that narrows the subarticular
portion of the spinal canal. Measurement of the width of the
lateral recess with values of 2 mm and less are considered to be
pathological. Another possible point of compression of the nerve root is
a narrowing of the most distal part of the lateral recess, the
intervertebral foramen.
Degenerative spondylolisthesis
(pseudospondylolisthesis or degenerative anterior vertebral translation)
affects older patients, but is increasingly seen in middle aged patients,
even at the age of 40, the L4/5 segment being most frequently involved.
Sagittal orientation of the facet joints, surgical removal of the
inferior articular process and degenerative changes of the superior
articular process are the predisposing factors. Due to the
anteriorly oriented facet joints, the L5/S1 segment is rarely involved. Typically,
the degree of slipping in degenerative spondylolisthsis does not exceed
25%.
|
Degenerative
changes are primarily due to disc degeneration, which occurs with
ageing, infection or trauma. A degenerated disc leads to
narrowing of the intervertebral space and usually is accompanied by
spondylosis, with formation of spondylotic ridges. Degeneration
and loss of height of the disc occurs first in the posterior part. This
deformation of the disc, combined with the plane of orientation of the
facet joints leads to retrolisthesis of the cranial vertebra, which is
the most common form of degenerative vertebral translation. A
change in the relationship of the facet joints causes subluxation,
distension of the joint capsule and spondylarthrosis. Subluxation
of the facet joint occurs first and leads to symptoms only in a
lordotic posture. Degenerative listhesis may present as lumbar
instability, with or without stenosis. In the advanced stage it is
fixed, with a thickened capsule and joints, giving rise to permanent
symptoms.
|

|
|
Clinical
features:
|
Spondylolisthesis
|
Although a number of patients have permanent symptoms, the
majority of patients with lumbar spinal stenosis experience symptoms
while standing or walking. Symptoms or signs that occur while
walking lead to neurogenic claudication. Over some time of walking
distance shortens, sometimes so dramatically as to prevent the patient
making more than a few steps. Paucity of findings at physical
examination even in a patient with advanced symptoms is typical.
Permanent symptoms and signs unrelated to posture are caused
by a permanent compression of the nerve roots. Leg pain, motor
deficit sensory deficit and rarely, urinary dysfunction or impotence can
be found in this order of frequency.
Intermittent symptoms and signs occur while the patient is
standing, including low back pain, referred pain or back weakness.
These symptoms are related to a narrowing of the lateral recess while the
spine is extended. Therefore, symptoms are triggered or worsened in
postures that aggravate lumbar lordosis, including standing, walking,
especially downhill or downstairs, as well as while wearing shoes with
high heels.
Low back pain is a common complaint for a long time before
radicular compression occurs. Back weakness is a specific complaint
described by patients as if their back is going to give away, probably
caused by a proprioceptive sensation from vertebral joints and
muscles. Both complaints, as well as the referred pain
(pseudoradicular pain) are due to segmental instability of the spine and
are relieved by a posture that diminishes lumbar lordosis: leaning
forward while walking, standing, sitting or by lying down. While
walking, permanent symptoms can spread to previously unaffected
dermatomes or to the other leg, indicating involvement of other nerve roots.
Leg pain can even diminish, which is an unexplained phenomenon. Due
to postural widening of the foramina, some patients are able to ride a
bicycle without complaints, at the same time having intermittent symptoms
after only a short walking distance.
Neurogenic intermittent claudication is experienced by up to
80% of patients, depending on the severity of narrowing of the spinal
canal. Symptoms and signs leading to it are motor deficit, sensory
deficit, leg pain, in that order of frequency and rarely urinary
incontinence. Resting with the lumbar spine flexed lessens the
symptoms, but not resting in erect posture, in contrast t vascular
intermittent claudication. Neurogenic intermittent claudication is
caused by the insufficiency of vascular supply in one or more nerve roots
of the cauda equine occurring during motor activity and the increased
oxygen demand related to it. A focal area of deprived circulation
occurs at the point of mechanical compression, with neuronal
hyperexcitability that leads to pain or paresthesia. Demyelination
or loss of large neuronal fibres leads to weakness and numbness.
Another effect of mechanical compression is the archnoidal adhesions that
fix the nerve root and impair CSF circulation around it with a negative
impact on its metabolism.
Imaging:
Plain X-rays in anteroposterior, lateral
and oblique views are useful in showing lumbarisation or sacralisation,
in determining the shape of the intervertebral formina and the facet
joints, showing spondylosis, spondlarthrosis, retrolisthesis,
spondylolysis and spondylolisthesis. Central spinal stenosis or
lateral recess stenosis cannot be quantified by this method.
Myelography (out dated now) was helpful in
determining the degree and longitudinal extent of stenosis because more than
one point of compression may be insufficient.
CT is the best method to evaluate osseous
compression and at the same time other structures are visualized.
With 3 mm thick slices the size and shape of the spinal canal, lateral
recess, facet joints, laminae, as well as the morphology of the
intervertebral disc, epidural fat and ligamentum flavum are shown.
MRI is clearly superior to CT in the
visualization of non-osseous structures and currently the best method for
evaluating the contents of the spinal canal. Despite this, apart of
showing disc degeneration in T2-weighted images, it usually does not add
substantial information necessary in the diagnosis of lumbar spinal
stenosis. However, considering the rapidly growing experience with MRI,
which is a non-invasive method the role of MRI in the diagnosis of this
disease, will increase. Especially a possibility of performing
functional sequences of the lumbar spine would be very valuable.
It is very important that all radiological findings are
correlated with the symptoms, since asymptomatic narrowing seen on MRI or
CT is often found, either as stenosis of an asymptomatic segment, or in
completely asymptomatic patients and should be ignored.
Treatment:
The treatment has to be adapted to the patient, his age and
aims. In the majority of patients a significant improvement or a
relief of symptoms can be achieved. Radicular symptoms and
neurogenic intermittent claudication are more likely to resolve with
treatment than back pain, which persists in up to one third of patients.
Conservative treatment consists of
analgesia and wearing a lumbar corset which by alleviating lumbar
lordosis can lessen symptoms and increase the walking distance. For a
group of patients the relief they experience is satisfactory and the
walking distance suffices for their daily needs.
A trial of three months’ duration is recommended as
the initial form of treatment, unless motor deficit or progressive
neurological deficit is present. Conservative therapy of lumbar
spinal stenosis with permanent symptoms is rarely successful on a long
term basis, in contrast to conservative therapy of a herniated disc.
Surgical treatment is indicated if
conservative therapy fails, and in the presence of incapacitating
permanent symptoms, especially a motor deficit. Depending on the
clinical symptoms and signs, and partly due to a different approach to
lumbar spinal stenosis three groups of operative procedures are performed:
·
decompression operations
·
combined decompression and stabilization of unstable motion segments
·
operative stabilization of unstable motion segments alone.
The decompression procedures are: decompression of the
spinal canal, decompression of the spinal canal with decompression of the
lateral recess and the intervertebral foramen, selective decompression of
the nerve roots.
1)Decompression of the Spinal Canal
Laminectomy is the standard method of
decompression of the central part of the spinal canal. The
advantages are that it is usually easily performed and has a high initial
success rate. The failure rate with recurrence of symptoms was one fourth
of patients after 5 years in one study. There is a relatively low rate of
non-specific postoperative complications and epidural scarring.
Traditionally, laminectomy alone was thought not to impair
the stability of the lumbar spine, as long as the other structures of the
spine were intact, particularly in older patients. In a degenerative
spine other important elements such as the intervertebral disc and facet
joints are often impaired. This might explain the occurrence of
postoperative spondylolisthsis after laminectomy, which leads to a poor
result.
If laminectomy is performed in the presence of degenerative
spondylolisthsis or if it is combined with operative impairment of the
disc or the facet joints there is a high incidence of postoperative
instability. Preservation of the disc, even of a degenerated one, seems
to help segmental stability (Goel, 1986). It is for this reason
that discectomy is not recommended in lumbar spinal stenosis in which the
symptoms are precipitated through a disc protrusion or herniation, unless
the herniated disc compresses the nerve root even after decompression of
the lateral recesses.
Epidural scarring occurs after laminectomy and is sometimes
located in the next, non-operated segment. If scarring is very
pronounced, it is termed ‘postlaminectomy membrane’. Fat auto
transplants are applied epidurally by some surgeons in an attempt to
reduce fibrosis. While some results seem to support this,
postoperative swelling of fat can result in nerve root compression.
If decompression has to be performed in a patient with
osteoporosis, it should be very limited, since eventual postoperative
instability is difficult to treat.
Laminectomy with partial facetectomy is
the standard procedure in the treatment of spinal canal stenosis
associated with lateral recess stenosis. It is seldom that a pure
laminectomy is sufficient in spinal canal stenosis, so it usually has to
be combined with some form of partial facetectmy. “unroofing” of
the vertebral foramen in the strict sense of the word can be performed
only from a lateral approach, as for an extraforaminal herniation of the
disc.
Another infrequently used possibility is the wedge
procedures (laminoplasty), with removal and reinsertion of
the laminar arches and spinous process.
2)Selective Nerve root decompression:
Unless a pronounced narrowing of the sagittal diameter of
the spinal canal exists, a selective nerve root decompression can
suffice, especially if the patient has strictly unilateral symptoms. A
medial facetectomy through a laminotomy can be performed. Usually
the medial portion of the facet joint that overlies the nerve root is
removed. Specific complications of the procedure include insufficient
decompression, instability caused by a removal of 30%-50% of the facet
joint, or a fatigue fracture of the thinned pars articularis.
3)Decompression and stabilization:
Laminectomy can be combined with various methods of
stabilization. Newer systems using pedicular screws, as well as
older systems like the Knodt rods, Harrington rods, and the Luque frame
with sublaminl wiring are used.
In degenerative spondylolisthesis laminectomy and
intertransverse process fusion with or without internal fixation is
thestandard procedure, posterior lumbar interbody fusion and anterior
interbody fusion are alternatives. Laminectomy with spinal fusion,
some claim, is superior to laminectomy alone, since laminectomy alone was
associated with a high incidence of progressive spondylolisthsis.
Complications of stabilization procedures include breakage
of osteosynthetic material, neurovascular trauma, fractures of the
spinous process, the laminae or the pedicles, pseudoarthrosis, paralytic
ileus, and pain at the iliac graft donor site. Degeneration and
postfusion stenosis at the next motion segment to a fusion caused by
hypermobility may occur. Although experimental results support this
theory, the clinical effects of this complication are unknown.
Apart from degenerative spondylolisthesis where
decompression and stabilization is the recommended procedure, there is no
consensus as to the most effective treatment. Lumbar spinal
stenosis is treated operatively in a large number of series, with
favorable short term results. However, after more than 40 years of
research and experience in treatment the etiology is not fully
understood. In addition, definition and classification are
difficult because the degree of stenosis does not always correlate with
symptoms.
A recommended surgical protocol is
·
in patients who have permanent symptoms that increase on standing or
cause neurogenic intermittent claudication decompression and
stabilization,
·
in patients who have no permanent symptoms but clearly posture related
intermittent symptoms a stabilization procedure, especially if there is
relief with a lumbar brace.
Weight reduction, and
exercises to improve posture and strengthen abdominal and spinal
muscles
must accompany any form of
treatment, surgical or conservative.
|
