|
The skull bones are affected by lesions similar to
those seen in the other bones, such as benign or malignant neoplasms or
metastatic deposits, congenital dysplasias, metabolic disorders, and
hemopoietic disorders. The vault of the skull is made up of membrane
bones whereas the base is of cartilaginous origin.
It has been reported that the primary skull tumors
account for 0.8% of all bone tumors. The vault is made up of membrane
bones whereas the base is of cartilaginous origin. This influences the
pathology. Lesions that are primarily intracranial may involve the
skull secondarily, and similarly, skull tumors can spread
intracranialy.
Clinical features:
Swelling and local pain are the usual presenting
symptoms. Associated neurological deficit suggests intracranial
extension.
They produce symptoms by expansion of the skull or
compression of the adjacent brain or venous sinuses.
Skull base lesions can invade or compress the
cranial nerves. Headache and/or focal bony pain may result. When
cerebral venous thrombosis occurs secondary to compression or invasion,
the abrupt or insidious onset of headache is related to elevated
intracranial pressure.
The site of skull base lesions can often be
localized by the cranial nerve deficits. There are five clinical
syndromes:
The orbital syndrome is characterized by
progressive supraorbital pain over the affected eye and visual
blurring, followed by diplopia. On examination, there is proptosis of
the affected eye and external ophthalmoplegia; there is variable
numbness in the first division of the trigeminal nerve and pre-orbital
swelling.
The parasellar or cavernous sinus
metastasis syndromes are characterized by a severe, unilateral frontal
headache and diplopia. There is paresis of either or both of the
oculomotor and abducens nerves, numbness in the first division of the
trigeminal nerve, and possibly papilledema. There is no
proptosis.
Presenting complaints in those with middle
fossa (gasserian ganglion) syndrome are numbness, paresthesias, or
pain in the area innervated by the second or third division of the
trigeminal nerve. Headache is uncommon.
Involvement of the jugular foramen produces
hoarseness or dysphagia and often retroauricular pain. Examination
reveals evidence of glossopharyngeal, vagus, and accessory nerve
dysfunction.
In contrast, patients with the occipital
condyle syndrome present with severe unilateral occipital pain,
exacerbated by neck flexion and associated with neck stiffness, pain over
the occipital area, and unilateral hypoglossal nerve paralysis.
Diagnosis:
CT scan has mostly replaced plain
x-rays. It provides accurate information regarding the involvement of
the skull bones as well as the intracranial and extracranial soft
tissues. Contrast studies assess the vascularity and the involvement of
dural venous sinuses.
MRI scan provides better
delineation of soft tissue involvement. As compact cortical bone lacks
in unbound protons, the inner and outer tables appear as a signal void.
The diploe has abundant fat and hence images well. It is specially
useful in skull base lesions Contrast-enhanced MRI of the skull base
that can detect soft tissue abnormalities and provide excellent
visualization of the cavernous sinus and cranial nerves.
Cerebral angiography has limited
indications.
Management:
Surgery, radiotherapy, and chemotherapy are often
used in combination as in other bone tumors.
Surgery depends on
the suspected nature and the site as well as intracranial involvement.
Needle biopsy is a simple out patient procedure and may provide a clue
on pathology. Primary lesions, ideally, are excised completely whenever
possible. Cranioplasty may be done at the same sitting or at a later
stage. Skull base lesions may need special exposures and involvement of
plastic and ENT surgeons.
Even when complete excision is not possible,
surgical palliation may be considered to avert neurological or
life-threatening events, especially in patients whose prognosis is
uncertain. Surgical debulking of a mass lesion may allow for more
effective chemotherapy and radiation therapy.
Radiation therapy,
either curative or palliative, is the mainstay for malignant tumors.
Multiple small fractionated doses per day spread out over a longer
time, is more effective with less damage to normal structures.
Generally, the required dose is 55 Gray or 5500 rads in 30 fractions
over six weeks utilizing megavoltage photon radiation. There is 1% risk
of delayed sarcoma in the irradiated bone. Higher energy photon or
electron beam therapy is ideal and can be tailored to the tumor volume
by computerized techniques.
Chemotherapy alone is
useful in a few, such as, lymphomas. Currently, it is used as an
adjuvant to other forms of therapy and as a palliative therapy.
Primary skull tumors:
a) Benign skull tumors:
Osteomas are the
commonest (about 30%). They arise from membranous bone and proliferate
into dense cortical or spongy cancellous bone. The frontal and mastoid
air cells are common sites. These slow growing tumors form an outward
excrescence which is hard and painless and are usually noted while
combing the hair. A compact osteoma may become hard like
ivory. The attachment to the skull may be narrow or broad.
Rarely, an osteoma may extend intracranially and cause seizures.
In plain X-rays, an osteoma is seen as a solid
homogenous bony shadow. There are no increased vascular
channels. Tangential projections reveal the base and the absence
of involvement of the diploid and inner table. When the inner
table is involved, differentiation from a meningioma becomes
necessary. CT gives the precise diagnosis. Myltiple osteoma of
the calvaria and mandible with soft tissue tumors of the skin and
colonic polyposis form the triad of Gardner’s syndrome.
Microscopically, the tumor is a nucleus of osteoid tissue in a
background of osteoblastic connective tissue and is completely enclosed
by reactive bone. Histological differentiation from fibrous
dysplasia is difficult: but the presence of smooth, homogeneous and
sharply defined sclerotic nodules is unusual 0in fibrous dysplasia.
Osteomas are surgically curable. The indications
for removal are rapid growth, pain, obstruction to sinus out lets and
noticeable deformity. Small osteomas of the outer table may be
resected easily without destruction of the inner table. As these
lesions are very hard, it is wiser to remove them by cutting around
their base through the cancellous tissue. A large lesion needs
removal of the entire bone as a flap and the defect is closed by cranioplasty.
After excising the bone flap. The osteoma can be excised from the flap
and the flap can be autclaved and used to close the defect primarily.
Hemangiomas constitute
about seven per cent of all skull tumors. About two thirds of
haemangiomas of bone occur in the skull or the vertebral column.
They arise from the vascular elements of the diploe, mainly in the
vault of the skull and to a lesser extent in the roof of orbit or
petrous temporal bone. They are slow growing and may reach a
large size. They are painless and the presence of a swelling is
the chief complaint. The swelling is hard, but may be soft in
some places. The skull is involved by erosion and the margins are
imperceptible. Dilated veins may be present. In haemangiomas of the
orbit, proptosis, blindless or extra ocular palsies may be seen.
Haemangioma of the petrous bone may present with deafness and cranial
nerve palsies.
The plain X-rays show a swelling with a typical
honeycombed or sunburst appearance. The diploe is enlarged and
both tables of the skull bulge, outer more than the inner.
Rarely, intracranial extension is seen. The trabeculae are seen
vertically oriented. The edges are well defined and a thin margin
of bony condensation may be evident. CT images with “bone window”
show the hypodense matrix with discrete, thickened, sclerotic and
widely separated trabeculae. Despite the vascular nature of the
lesion, contrast enhancement is an exception rather than the
rule. Carotid angiography shows enlargement of the external
carotid artery branches. Rarely, there may be an internal carotid
supply to these tumors.
Treatment is usually by enbloc excision or wide
curettage. The tumor appears as a blue domed hard mass under the
pericranium. Sometimes the dural surface may bleed profusely in
which case circumferential incision of the dura and resuturing will
help. Radiotherapy is advisable in situations where excision is not
feasible. Doses up to 30 Gy(3000 rads), in three weeks, may be
required.
Giant cell tumors (osteoclastoma) arise from
the cartilaginous bone in the sphenoid, mastoid or occipital
areas. They are extremely rare in the bones of the vault, as
osteoclasts are not usually present in membrane bones. Their
pathogenesis is unknown, although trauma and hemorrhage may precede their
occurrence.
Osteoclastoma of the skull presents as a painless
bony swelling and radiographs show evidence of rarefaction or
destruction of bone. Excision is the treatment of choice; but it
is often incomplete and needs supplementary radiotherapy to ensure
freedom from recurrence. Occasionally, malignant changes have
been reported after surgery and radiotherapy.
Epidermoid and dermoid tumors of
developmental origin are derived from epithelial cell rests ectopically
included in the bone during development. They are commonly seen
in or near the midline in the vertex, the frontal or occipital regions
or in the temporal bone. However, they may occur anywhere in the
clavarium. They originate in the diploe and enlarge in the both
directions expanding and thinning both the tables by continuous growth
pressure. The bone at the edge of the lesion gets
sclerosed. The lesion may break through the egg shell thin tables
and expand under the scalp or extradurally. The swelling under
the scalp is firm, rubbery and non-tender. Sometimes a tract may extend
through the inner table and dura to end in an intradural lesion. A
lesion in the midline especially over the torcula may involve the
venous sinuses. Very large intracranial extensions may exist with
surprisingly normal intracranial pressure and with no neurological
deficits. These are described as giant intradiploic
epidermoids. The larger lesions, especially epidermoids, tend to
get infected and osteomyelitis may result.
Plain radiographs show a clear cut area of
radio-lucency in the skull sclerosed margins resembling an emissary
foramen. Tangential views show expansion of the tables. CT
accurately delineates the bony defect and the size, location and
extension of the soft tissue mass outside and inside the skull and
dura. The lesion appears hypodense relative to the adjacent
brain, due to the contained keratinized debris and cholesterol.
They do not enhance with contrast, but adjacent compressed brain shows
marginal enhancement. On MR these lesions appear hyperintense in
T2 weighted images and most often hypointense in T1weighted images.
Treatment is by surgery. Pure extracranial lesions
can be excised enbloc. A careful search must be made for any
intradiploic or intracranial extension along a thin track which,
if present, needs to be excised. While dealing with midline
lesions the surgeon must be prepared to do an extensive craniotomy and
venous sinus repair if necessary.
Chondromas arise mainly
in the cartilaginous bones of the base of the skull. They
commonly occur between the ages of 20 and 40 years. The common
sites are the paranasal sinuses and the spheno-ethmoidal and
spheno-occipital extended into the sellar or parasellar region,
producing visual and ocular nerve palsies or endocrine dysfunction. The
posterior lesions may compress the brainstem and involve the lower
cranial nerves. Radiographically, a chondroma appears a lytic
lesion at the base of the skull with fairly sharp margins. Areas of
stippled calcification maybe seen in more than 60 per cent. CT
reveals well marginated bone destruction and an associated homogenous,
isodense and lobulated soft tissue mass with interspersed
calcification. Contrast enhancement is infrequent and when
present is minimal.
Sarcomatous changes occur in one to two per cent
of these tumors, more frequently in individuals with Mafucci’s syndrome
(multiple enchondromas and multiple subcutaneous hemangiomas). Rapid
growth indicates a malignant change. Histologically, malignancy
is deduced by the presence of atypical cartilage cell nuclei in the
actively growing peripheral portions of the neoplasm. The
treatment of a chondroma is total removal wherever possible. Most
often only partial removal is possible, especially at the skull base.
Decompression of neural structures by such partial removal is often
beneficial.
Aneurismal bone cyst is a
multiloculated expanding cystic tumor with a rich vascular network in
the walls. The encircling inner and outer tables are eroded to
form thin bony shells. Some cysts show a central core of
hemangioma and repeated hemorrhage may be the cause of the cystic
expansion of the skull tables. These lesions may either becomes
symptomatic or enlarge during pregnancy. On CT, the contents of
the cyst may be of the fluid. The superficial temporal and middle
meningeal arteries supply the tumor and this is made out well on
selective external carotid angiography.
Ossifying fibromas (benign
osteoblastoma) are a rare solitary, vascular tumor predominantly
osteolytic in character with varying degree of calcification and new
bone formation. Treatment is local excision.
Osteoblastomas are seen occasionally in the
base of the skull, but rarely in the vault. Depending on the site of
origin, they produce signs of pressure on the optic nerves, the
pituitary, the hypothalamus, the brainstem and other cranial nerves.
Radio logically, islands of erosion with normal bone in between are
seen. Local excision and post operative radiotherapy is the usual
practice.
b) Malignant tumors:
Chondrosarcomas are rare, usually in adults, as
a malignant transformation in a benign chondroma. The common site is
the base of skull, in and around the sella, CP angle, or the
fronto-ethomoidal sinuses. They grow for a long time and produce
pain, deformity, and cranial nerve palsies. CT reveals an irregular
destructive process with a homogenous, hyperdense, and enhancing soft
tissue mass. Radical resection and radiotherapy is the traditional
treatment. They are locally invasive and tend to recur.
Osteogenic sarcomas are rare; it
occurs usually in the young and in the vault. Occasionally, it occurs
as a late complication following radiotherapy. They grow rapidly and
metastasize to the lungs and other bones. CT shows an enhancing
irregular, heterogenous extradural mass with prominent new bone
formation. Radical excision and radiotherapy is recommended. Adjuvant
chemotherapy helps.
Fibrosarcomas arise from the periosteum of
the skull or the dura. They are rapidly growing and painful. X-rays
show thinning of the outer table with irregular margins and an
overlying soft tissue mass. Radical excision and post–op radiotherapy
is advised. Chemotherapy has no role.
Chordomas are slow growing, locally invasive
and of embryonal origin from the remnants of the chorda dorsalis. The
smaller ones are pedunculated, the larger ones are diffuse. The usual
sites are at the skull-base, in the sella, the clivus, and the
nasopharynx. The sixth nerve is commonly affected. Brainstem
compression occurs later. CT and MRI show a soft tissue mass in the
midline with bone destruction. Occasionally (10%) there may be a
sclerotic response. Extended skull base approaches may be needed for
satisfactory excision. Post–op radiotherapy is advised.
Other rarer tumors, such as, reticulum cell
sarcoma, angiosarcoma, malignant fibrous histiocytoma can occur. The
diagnosis is usually made on histology. Wide excision and radiotherapy
is advised.
|
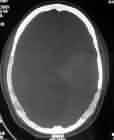
Skull metastases:
Hematogenous metastases are usually from
the breast, the lungs, the prostate, the thyroid, and the kidney.
Though metastases can affect any part of the skull, vault is the
common site. They are usually osteolytic, except when the primary is
from the prostate, when it is osteoblastic. Radiologically they
appear as multiple, poorly marginated areas of slightly increased
density. Occasionally in some cases of breast cancer, the skull
metastases may appear as mixed lucent and sclerotic areas. Plain
xrays are positive in 60% of cases and CT in 85%. Extradural and
scalp extension may show as areas of contrast enhancement. Isotope
scans are more sensitive. Biopsy may be needed to confirm the lesion.
Treatment is correlated with that of the primary.
Lymphomas of bone are a common feature in
disseminated lymphomas and occur in 10-15% in Hodgkin’s and 7-25% in
non Hodgkin’s. The more aggressive lymphosarcoma and reticulum
sarcoma rarely involve the skull. Treatment is local radiotherapy and
chemotherapy.
Leukaemias appear as ill-defined areas
of rarefaction with peripheral new bone formation similar to neuroblastoma.
Low dose radiotherapy and chemotherapy of the systemic disease is
recommended.
Multiple myeloma affects the
males more commonly between 40-60 years of age. Skull x-rays show
multiple punched out areas of bone destruction. Biopsy or bone marrow
biopsy may be needed to confirm. They are treated with chemotherapy.
Occasional solitary plasmocytomas are treated with radiotherapy.
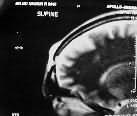
Neuroblastoma is a common tumor of
childhood. Skull metastases often precede the detection of the
primary adrenal tumor. Diffuse nodular lucencies are seen
radiologically. They are highly vascular and lift up the periosteum,
producing radial bone speculation extending into the soft tissues.
The dura often resist the spread; however, occasionally, an
intratumoral hemorrhage may rupture into the brain parenchyma.
Spontaneous resolution into a more benign form has been reported;
skull metastasis suggest a poor prognosis. Local radiotherapy and
systemic chemotherapy is the treatment of choice
|
|

|
|
Skull metastases from Ca. breast
|
|

|
|
Multiple myeloma
|
|

|
|
Olfactory Neuroblastoma-MRI
|
|
Ewing’s
sarcoma
are often multicentric in origin involving the tibia, ribs, and
vertebrae and rarely seen as a primary skull lesion. Local radiotherapy
and chemotherapy is recommended.
|
Skull involvement by
direct extension:
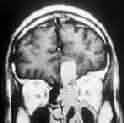
Meningiomas may produce
varying degrees of incidental bony changes in the overlying skull and
may also invade the skull bone itself and may break through the outer
table to present as a subcutaneous swelling. The involved bone is
considerably vascular with tortuous arterial and large venous
channels. The bony changes may resemble those of fibrous dysplasia.
Sometimes, they remain entirely intra-diploic, expanding the two tables
resulting in a doughnut like lesion. Occasionally, there may be bone
destruction similar to that of a metastasis.
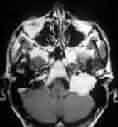
Benign Nasopharyngeal tumors
usually become symptomatic long before the skull involvement.
Angiofibroma and squamous cell pappilloma are the common ones. Marked
intracranial extension may require combined approach with ENT
surgeons. The malignant tumors of the nasopharynx and the paranasal
sinuses usually present with intracranial involvement and are treated
with radiotherapy following biopsy.
Glomus jugulare is
discussed elsewhere.
Conditions simulating skull tumors:
Osteomyelitic changes appear radiologically
long after the onset of clinical signs and symptoms. Multiple nodular
lucent areas appear in the outer table or diploe. Later they condense
into a large defect with scalp edema (Pott’s puffy tumor). Poorly
defined sclerosis occurs at the edges of the bone with practically no
subperiosteaL new bone or sequestrum formation.
Leptomeningeal
cyst
as complication of growing fracture is children may mimic a tumor
radiologically as a lucent area with scalloped marigins and a soft
tissue shadow outside the skull. Occasionally, it may be in between
the tables producing intraosseous cyst.
|
|

|

|
|
Meningioma with skull infiltration-MRI
|
Intradiploic meningioma-MRI
|
|

|

|
|
Nasopharyngeal Angiofibroma-MRI
|
Nasopharyngeal tumor with parasellar
extension-MRI
|
|
|
|
|
Ethmoidal
tumor
with
intracranial extension-MRI
|
Glomus jugulare tumor.-MRI
|
|
Cephalhematoma in the new born, following
forceps delivery, may produce a soft tissue shadow radiologically. It
is commonly seen in the parietal bone limited by sutures and mimics a
tumor. Calcific edges gradulally project into the soft tissues of the
scalp, resulting in a shell like calcification. Rarely, a deformity
persists.
Paget’s disease (osteitis deformans) is
multicentric involving pelvis, the femora, the vertebrae, and more
commonly the skull. Men are more frequently involved. It starts as a
diffuse mottled thickening in the frontal or occipital area as
irregular patches or lysis which give the appearance of a geographical
skull radiologically. Later, patchy sclerosis develops. Deafness and
blindness due to foraminal involvement may occur. Except for neural
decompression, there is no specific treatment. Sarcomatous change is infrequent.
Sarcoidosis rarely involves the skull. It is seen
as multiple punched out areas of rarefaction.
|
Eosinophilic granuloma shows an
irregular area of of rarefaction with no sclerosis in skull
radiologically. Complete excision and small dose radiation (10Gy), is
curative. The multiple recurrent type is seen n children, often
involving the frontal bone and spreads extensively showing clear cut
but irregular edges described as ‘ map like’. The facial bones and
paranasal sinuses eventually get invoved. Local radiation following
biopsy. And chemotherapy is recommended.
Fibrous dysplasia is a benign
disorder of bone commonly seen in the young. Normal osteoid is
replaced with connective tissue with varying osseous metaplasia. The
cystic type affects the vault, and type involves the base.vault, the scleothe
sclerotic type involves the base. The mixed type is rare.
There is need for any specific treatment, but for decompression
if there is neural compression. Sarcomatous change is rare.
Mucocoele occurs in any of the paranasal
sinuses, commonly in the frontal, due to outflow obstruction in the
sinus cavity. The walls bulge and may burst through the dura. A
sphenoidal lesion may erode the optic foramen. The floor of the sella
may bulge upwards. Ethmoidal lesion may produce proptosis. Complete
excision with all the sinus lining is advised.
Sinus pericranii is a
congenital skull defect, containing abnormal emissary veins which
connect an intracranial venous sinus, commonly the superior sagittal
sinus in the frontal region with a cluster of veins or a venous
angioma in the extracranial space. Typically, the veins bulge as a
swelling in the recumbent posture and disappear in the erect
posture.
|
|

|

|
|
Eosinophilic granuloma
|
Eosinophiliv granuloma-CT
|
|
|
|
|
Fibrous dysplasia-CT
|
Sinus pericrani-MRI
|
|

|

|
|
Sphenoidal mococoele-CT
|
Sphenoidal mococoele-MRI
|
|
|
