|
Venous angiomas
Venous
angiomas are also known as "Developmental
venous anomalies" (DVAs) to emphasize their frequency and their benign
nature and low incidence of sequelae. They are the most common vascular
malformation found at postmortem.
They are most commonly located in the following descending
order of frequency frontal lobe, parietal lobe, and cerebellar
hemisphere. They may also be found in the region of the vein of
Galen
They are sporadic in nature with no genetic predisposition
They occur due to arrest of normal venous development with
retention of primitive medullary veins draining blood into a large
anomalous draining vein is the presumed etiology
Pathology
They are mostly seen as a small single lesion of low flow
and low pressure. They represent the venous drainage of the area. There is
anomalous venous drainage of otherwise
normal brain tissue. It consists of radially arranged anomalous medullary
veins that converge on a larger central draining vein that, in turn,
drains into deep or superficial venous system.
The "crown" of veins that converge onto the
connecting trunk are "collecting veins" that drain the
capillaries from the affected volume.
The veins are slightly thickened and hyalinized with large
amounts of smooth muscle and elastic tissue. Venous radicles are
separated by normal/ gliotic intervening brain tissue.
No abnormal arteries are found. They may be associated with
a cavernous angioma in 20%.
Clinical features
They are most commonly detected incidentally. However they
may present with headache and focal deficit. Seizures occur rarely and
may be due to chronic ischemia, encephalomalacia and calcification .
Bleeding in a venous angioma is seen less commonly than
seizures.
Hemorrhage, however, may be more frequent in those venous
angiomas with concurrent stenosis of the draining vein and or concurrent
cavernous angioma. Even in these cases the bleed is mostly at the sites
of the cavernoma and not the venous angioma
Investigations
CT SCAN
Non contrast scan is normal unless there is calcification or
acute hemorrhage
Contrast enhanced scan reveals a tuft of small vessels
draining into a dilated, subependymal or subpial vein may be seen with
contrast.
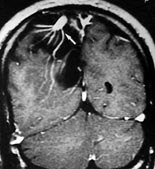
MRI
It reveals transmedullary flow voids or as paired
transmedullary lines of increased and decreased signal representing
spatial misregistration of the vessel wall and lumen because of the
Doppler shift in frequency associated with flow. The draining trunks are
substantially larger than adjacent veins, perhaps because they serve as
collateral drainage pathways for adjacent regions in which veins failed
to develop (or later thrombose).
Gadolinium enhancement improves display of slow flow and may
be required to detect venous angiomas not otherwise seen. It reveals the
characteristic medusa head draining into a larger vein.
Stenosis of the large central vein as it enters the dural
sinus and concurrent cavernous angiomas must be sought out and described,
if possible, since they may signify increased risk of bleeding.
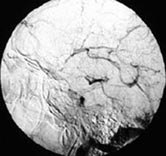
ANGIOGRAPHY
Occasionally may be angiographically occult, however, they
classically produce distinct caput medusae (other descriptive terms
include: a hydra, spokes of a wheel, a spider, an umbrella, a mushroom or
a starburst pattern or "medusa head")
It really looks more like a hydra or a palm tree - the
dominant transcortical vein is the trunk; and the radiating crowns of
feeding veins are the leaves.
|
|

|

|
|
|
Post contrast MRI-T1-cor
|
Rt.carotid angio-AP
|
Temp ICH-CT
|
Temporal venous angioma-angio
|
Management:
Because of the following reasons Rx is rarely indicated.
Surgery is reserved for the following situations
-
Documented bleeding
-
Intractable seizures attributed to the lesion
Radiosurgery is still debatable. It is not accessible via an
endovascular approach
Prognosis:
Excellent unless there is associated venous stenosis or
cavernoma
Capillary telangiectases:
These lesions consist of groups of abnormally swollen
capillaries and usually measure less than an inch in diameter.
Capillaries are the smallest of all blood vessels, with diameters smaller
than that of a human hair; they have the capacity to transport only small
quantities of blood, and blood flows through these vessels very slowly.
Because of these factors, telangiectases rarely cause extensive damage to
surrounding brain or spinal cord tissues. Any isolated hemorrhages that
occur are microscopic in size. Thus, the lesions are usually benign.
However, in some inherited disorders in which people develop large
numbers of these lesions, telangiectases can contribute to the
development of nonspecific neurological symptoms such as headaches or
seizures
AOVMs:
Purists claim that angiograpically occult venous
malformation (AOVM) is a heterogenous group of malformations
(AVMs, cavernomas
and others) that are not detected by angiography and diagnosed by CT or
MRI. They do not group them with the Capillary telangiectasis and Cryptic
AVMs, which are a separate histopathological entity, encountered
during haematoma evacuation. For all practical purposes they are
considered as one group by most. Surgical intervention is indicated only
when there is a large haematoma, requiring evacuation.
|
