|
Venous infarct is an elusive diagnosis because of its
nonspecific presentation and its numerous predisposing causes. Cerebral
venous infarcts constitute less than 1% of acute strokes. It occurs is in areas atypical for
arterial vascular distribution.
The true incidence is not known, but rarer than other types
of stroke with a slight female preponderance, accounting up to 50% of
strokes during pregnancy and puerperium. It is more common than
previously thought. Increased frequency is being reported since advent of
DSA (digital subtraction angiography), CT & MRI/V.
Pathophysiology:
|
Cerebral venous thrombosis results from occlusion of a
venous sinus and/or cortical vein and usually is caused by a partial
thrombus or an extrinsic compression that subsequently progresses to
complete occlusion. Once the vein is occluded, the clot propagates into
the cortical veins, leading to the obstruction of cortical venous
drainage. Venous pressure increases, and causes breakdown of the
brain-blood barrier with vasogenic edema and hemorrhage. Finally,
venous infarct with cytotoxic edema ensues. The cerebral cortex is
edematous with petechial or gross hemorrhages. Involvement of the deep
cerebral veins (eg, basal vein of Rosenthal) can progress to bilateral
thrombosis of the internal cerebral veins with thalamic hemorrhagic
infarction.
Hemorrhage or infarct
(non-arterial distribution) occurs due to elevated venous and capillary
pressure.
Usually the onset of symptoms is gradual
(weeks).
Acute (days) or insidious (months)
onset are not uncommon.
|
|
Distribution of venous thrombosis
|
|
Multiple
vessels
>70%
Superior sagittal
sinus
72%
Transverse
sinus
70%
Right
26%
Left
26%
Both
18%
Straight
sinus
14%
Cavernous sinus
3%
Cerebral
veins
38%
Superficial
27%
Deep
8%
Cerebellar
veins
3%
|
|
Risk
factors:
As many as 25% of patients present with no predisposing risk
factor.
Multiple pathophysiologic mechanisms and predisposing
factors exist, including the following:
1) A low-flow state within the venous sinus due
hypercoagulable states is the most often detected cause.
They include,
Inherited
thrombophilias (in 1/3): Protein C / S deficiency,
Antithrombin III deficiency, Factov V Leiden mutation (with activated
protein C resistance), Prothrombin gene mutation,
Hyperhomocysteinemia, Paroxysmal nocturnal hemoglobinuria
2) Acquired causes:
Antiphospholipid
antibodies (lupus anticoagulant, anticardiolipin antibodies) with
or without associated with
SLE (lupus) or other connective-tissue disorders.
Dehydration (hyperosmolarity)
incl. Burns, diabetic ketoacidosis, Hyperviscosity (incl. Waldenstrom’s
Macroglobulinemia), Polycythemia, Sickle cell, Thrombocytosis.
Pregnancy &
puerperium
Malignancy
Inflammatory
bowel disease
Sarcoidosis
Nephrotic
syndrome
Oral contraceptive
pill, hormone
replacement therapy, heparin-induced
thrombocytopenia,
l-asparaginase
chemotherapy, corticosteroid therapy.
2) Local or distant infection account for 10% of the
patients, and include, mastoiditis, otitis media, paranasal sinus infection,
generalized sepsis, and facial or scalp cellulites.
3) Extrinsic compression or local invasion of a venous by
tumor are other possible causes.
4) Iatrogenic
causes include, invasive internal jugular venous catheters, post
craniotomy (esp. following excision of a convexity meningioma) transvenous pacemaker, Post
treatment of AVMs.
Clinical features:
|
The signs and symptoms of cerebral venous thrombosis
occasionally are nonspecific and highly variable, making the clinical
diagnosis difficult. Patients may have generalized or focal neurologic
symptoms and signs with features of raised ICT. Seizures are much more common that
with other stroke types.
Focal
neurological deficit is seen in up to 2/3 of patients.
They may be
bilateral alternating deficits (4%).
Rapidly
progressive decreased LOC, headache, nausea, pyramidal signs (rarely),
the so-called “Catastrophic presentation” may
mimic SAH.
Psychiatric
disturbances may be seen.
|
Headache
75%
Papilledema
49%
Motor or sensory
deficit
34%
Seizures
37%
Change in
LOC
30%
Dysphasia
12%
Multiple cranial
nerve palsies 12% Cerebellar
incoordination
3%
Nystagmus
2%
Hearing
loss
2%
|
|
Imaging studies:
CT reveals hyperdense dural sinuses and
rarely cortical veins, related to the presence of clot within the
lumen. Hyperdense petechial hemorrhages and hypodense edema may be seen
in the cortical grey matter and subcortical white matter. On
noncontrast CT scan, the classic finding is the delta sign, which is
observed as a dense triangle (from hyperdense thrombus) within the
superior sagittal sinus. However, this is not specific, since high
attenuation in the healthy nonthrombosed sinus can be observed
occasionally and is common in neonates because of an elevated hematocrit.
On contrast-enhanced CT scan, the reverse delta sign (ie,
empty triangle sign) can be observed in the superior sagittal sinus
from enhancement of the dural leaves surrounding the comparatively less
dense thrombosed sinus.
The presence of both the delta and reverse delta signs
increases the likelihood of the diagnosis.
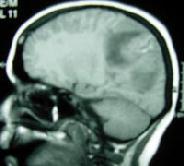
MRI is more sensitive in the detection of
venous sinus occlusion and venous infarcts. Acute clot is usually iso-
to mildly hyperintense on T1-weighted and hypointense on T2-weighted
images. Venous infarct develops in more than 50% of cases with dural
venous sinus thrombosis, characterized by gyral swelling and sulcal
effacement. The affected gyri are hypointense on T1-weighted and
hyperintense on T2-weighted sequences, however petechial or gross
hemorrhages are associated in the cortico-subcortical areas with
relevant signal intensity characteristics.
MR venography studies show the occlusion of cortical
venous sinuses with abnormal collateral channels.
|
|
|
|
Rt. parietal venous
infarct-MRI
|
|
|
|
Sagittal sinus thrombosis-MRV
|
|
MRI with MRV is preferred for diagnosis. Recently, CT
venography can also confirm the diagnosis.
Cerebral arteriography and venography may
be necessary when MRI scan and MRV are not available. Classic findings
are filling defects from thrombus within the venous sinus, and occlusion
of a draining sinus. Other findings include decreased focal venous
circulation around a thrombosed venous sinus, visualization of collateral
circulation, narrowing of arteries in the involved region, prolonged
contrast blush in the brain parenchyma, tortuous vessels in the capillary
and venous phases, and collateral flow in dilated anastomotic vessels.
Management:
Supportive management with IV fluids, anticonvulsants, and ICP control, as in acute arterial infarcts, is the mainstay.
The causative factor, such
as infection, needs urgent attention.
Anticoagulation
Goal is to arrest the
thrombotic process. IV heparin is recommended despite some reports to
suggest that anticoagulation do not add to recovery. It is generally
avoided, in the setting of ICH.
IV thrombolysis (local
urokinase) and endovascular thrombectomy may be considered when there is
clinical deterioration despite adequate anticoagulation. Oral
anticoagulation is continued for 3-6 months or life long if a
non-reversible prothrombotic condition identified.
Outcome:
Despite adequate measures, the reported the mortality rates
range from 6 to 20%.
Predictors of death or
dependency are: older age, coma or mental state disorder,
male sex, hemorrhage on admission CT scan, involvement of deep venous
system, presence of CNS infection and malignancy.
In
up to 80% of the patients there is no sequelae. 5% of them are severely
impaired at follow-up. 10% of them may recur.
About
15% of them develop venous thrombosis in another location (intra or
extracerebral).
Some
of the patients may progress to benign intracranial hypertension.
|
