|
Phakomatoses
is the coined by van der Hoeve in 1920, to describe a group of
hereditary neurological disorders that
have cutaneous and ocular stigmata. It is derived fro Greek root 'Phako'
meaning birth mark/mother spot. They are a group of disorders
characterized as dysplasias or neoplasms of organs derived from the
embryonic ectoderm. They have common features of neuroepidermal
maldevelopment and undifferentiated cells with disturbed patterns of cell
migration.
They are
commonly divided into:
1)
Neurofibromatosis, 2) Tuberous sclerosis, 3)von Hippel-Lindau disease, and
4) Neurocutaneous angiomatosis.
All
phakomatoses do not manifest ocular and cutaneous
findings;
VHL
shows no skin markers and the neurocutaneous
angiomatoses no ocular lesions.
Many similarities
exist between these groups, and several families have been reported with
overlapping manifestations of two phakomatoses. The genetic abnormality
in many of these disorders has not yet been identified
and the fact that stigmata of more than one
of these syndromes have been seen in the same patient could indicate that they are all due to an
abnormality in a small group of genes.
The
recognition of one of these syndromes in a patient mandates genetic
screening of other family members to provide genetic counseling. Finally, the CNS abnormalities can exist with out these disorders.
NEUROFIBROMATOSIS:
This is the commonest of the phakomatoses, with a reported incidence of one in 3000 births. It is an
autosomal dominant disease with high penetrance, but variable expression. This syndrome has been variously classified in literature, but recently
consensus is for two types which account for over 95% of all cases. Other cases of neurofibromatosis
represent either poorly expressed or variant
types.
|
Neurofilbromatosis-l
(NF-1):
NF-1 previously termed von Recklinghausen neurofibromatosis or peripheral neurofibromatosis, was
first described by von Recklinghausen,
in 1882. The genetic abnormality is
thought to be in chromosome 17 and is of extremely variable expression,
with members of the same family showing marked differences in clinical features.
A
diagnosis of NF-1 is made, if the patient fulfills any two of the following criteria:
a) Two or more neurofibromas of any type or
one plexiform neurofibroma
b) Six or more cafe-au-lait skin macules visible in room light,
each 5 mm or more in size in prepubertal patients; or,
15mm or more in post pubertal patients.
c) Two or more Lisch nodules.
d) Optic glioma.
e) Axillary or inguinal freckling.
f) Characteristic osseous lesions such as
sphenoid dysplasia or thinning of long bone cortices with or without
pseudoarthosis.
g) A first degree relative (parent, sibling or offspring) by the above
criteria.
Not all
the patients of NF-1 fulfill the criteria given above. These patients must be presumed to have
the NF-1 gene, but with poor gene expression.
1)
Cutaneous neurofibromas are characteristic of NF-1. These Schwann cell
tumors occur on the distal cutaneous nerve endings. They are most
numerous in the thoraco abdominal region, and the presence of
neurofibromas on the nipple or areola of the breast suggests an
association with pigmentation and / or hormones. They do not pose
any serious problem to the patient except
cosmetic, or rarely pain or itching. Operative removal of the lesion is done for painful or
irritant lesions or for cosmetic purposes.
2)
Plexiform neurofibromas may form along the
course of any nerve. While they grow mostly
from distal sensory nerves, they tend with growth to engulf major nerve
trunks and motor branches, rendering operative removal difficult with
attendant risks of a major neuro deficit. If it is asymptomatic, it is
best alone.
There is a
definite risk of malignant transformation in these patients. Neurofibrosarcoma
occurs in about five per cent of patients and is
the most dreaded complication of this disease. Treatment involves
amputation of the limb and major
resection, followed by radiotherapy and chemotherapy. However, 5 year survival rates are
only around 23%.
3) Lisch nodules arc pigmented hamartomas of the iris. They are present in
upto 94% of NF1 patients and seen, usually , after puberty.
4)Though spinal neurofibromas occur mostly on
the dorsal nerve root, the ventral roots may also he involved. These are often multiple and are most common in the cervical and lumbar regions. Surgery is necessary if cord compression develops.
The rare
occurrence of neurofibromas within the spinal cord, is seen more often in
case of neurofibromatosis than in the general population. Other spinal cord tumors are
not a prominent feature in NF-1.
5) Optic nerve gliomas occur in about
5-10 % of patients with NF-1. The
tumors behave like hamartomas and
the treatment is as for these tumors occurring in the general population. Brainstem and
post.fossa are other common sites. Hydrocephalus due to other tumors and
those due to aquedect stenosis are more common in NF-1.
6) Macrocephaly,
learning disorders, sphenoidal wing dysplasias, peudoarthosis,
pheochromocytoma and kyphoscoliosis are the other lesions in NF1.
|
|

|
|
Axillary
freckling with
large
cafe-au-lait spots
|
|

|
|
Giant cafe-au-lait spots
|
|

|
|
NF1with Rt.optic glioma
|
|

|
|
Plexiform
neurofibroma
with
palmar freckling
|
|
Neurofibromatosis-2 (NF-2):
This was previously called central neurofibromatosis or bilateral acoustic neurofibromatosis. It is an autosomal dominant disease, with the genetic abnormality on chromosome 22. Though the method of gene expression is not clear. It is much less common than NF-1.
|
The criteria for
the diagnosis of NF-2 are
a) Radiological evidence of bilateral acoustic neuromas
or
b)
a first degree relative with NF-2 and either a unilateral acoustic neuroma, or
two of the following: Neuro fibroma, schwannoma, meningioma, glioma, juvenile
posterior subcapsular cataract.
Patients
with NF-2 present with bilateral acoustic neuromas, which are for the
majority, symmetrical and present
with symptoms during adolescence and early adulthood.
|
|

|
|
Bil.Acoustic neuromas-MRI
|
|
|
A diagnosis of NF-2 should be suspected in any patient below 30
years of age, who has an acoustic neuroma, in a patient with multiple
meningiomas and in patients with Schwann cell tumors and minimal stigmata of NF-1. All
such patients and family members of NF-2 patients should be screened for
bilateral acoustic tumors with BAER, contrast enhanced high resolution CT and/or MR.
Patients
with NF-2 are liable to have other tumors including
multiple Schwann cell tumors on peripheral nerves,
spinal roots and cranial nerves, cranial and spinal astrocytomas and meningiomas. Treatment of
these patients is aimed at maintaining
brainstem and spinal cord function.
Surgery is offered for the larger tumors first,
while small tumors without any major pressure effects are kept under observation.
|
|

|
|
Small cafe-au-lait spots
|
|
TUBEROSE SCLEROSIS (Bourneville’s disease or Epiloia):
Von
Recklinghausen, in 1862, described association between
cardiac myomas and brain sclerosis.
Bournville, in 1880, correlated cortical tubers, seizure and mental
retardation, and called it ' tuberous sclerosis'.
Vogt Henrich, in 1908, described the clinical triad- adenoma sebaceum, seizures,
and mental retardation.
|
Tuberose sclerosis (TS) is an autosomal dominant
disorder with a variable penetrance. The
incidence is about 1 in 10,000 births and the extent of expression is very
variable. More than 60% are new mutation (i.e. no family history).
The
gene responsible is thought to be on chromosome 9q34 and 16p13.
Skin
manifestations:
Ash
leaf spots and other depigmented macules
are, best seen under a Wood's lamp (ultraviolet light).
Adenoma sebaceum
is an angiofibroma, a progressive lesion which develops after birth and
shows rapid growth around puberty. It has a
characteristic distribution, over the cheeks, nose, and chin, sparing the
upper lip and often confused for acne vulgaris.
Shagreen
or sharkskin patches are dermal fibromas which usually develop after 10
years of age. They occur mostly in the lumbosacral
region. They are not pathognomonic of TS and may occur in isolation.
Ungual
fibromas or Koenen's tumors are angiofibromas which occur in the lateral nail
groove,
along the proximal nail fold or under
the nail. They are more common in the toes than in the fingers.
Nervous system manifestations:
Cortical plaques (or tubers) and
subependymal glial nodules are
developmental hamartomas containing glial and
neuronal cell populations, which do
not enlarge once brain growth has stopped. There is no evidence of malignant transformation in these lesions. Degenerative changes take
place with gliosis and umbilication of
the cortex at the site of the tubers, leaving normal
brain in between.
Subependymal nodules (SEN), <1 cm in
size, are scattered along the entire wall of the lateral and third
ventricles. They are mainly glial hamartomas and contain calcium
deposits.
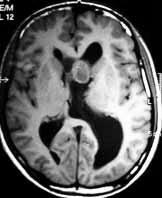
Subependymal 'giant cell astrocytomas' (SEGA) occur in about
10% of the patients with TS and do not develop from the subependymai nodules. These tumors react negatively to GFAP and are probably neuronal
in origin. They probably arise from the
germinal cell matrix which explains their vascularity. Anaplastic transformation is rare.
Calcified or hypodense lesions may also be
seen in the posterior fossa. They
may be GFAP positive or negative, but S-100and NSE positive.
No
isolated case of SEGA, without TS, has been reported.
|
|

|
|
Adenoma
sebaceum
|
|

|
|
Ungual
fibromas
|
|

|
|
Bil.Renal angiofibromas-MRI
|
|
|
|
SEGA-MRI
|
|
Lesions are also seen in other organs such as the
retina, heart, kidney and lungs.
In the eye, retinal hamartomas occur. They
rarely lead to visual problems.
Cardiac rhabdomyomas occur in
about 30% of patients; they may remain asymptomatic or may produce heart
failure in infancy. Renal angiomyolipomas are commonly found in these
patients.
Clinical features:
The clinical diagnosis of TS can be made by Vogt's
triad of seizures, mental deficit and adenoma
sebaceum.
The
disorder can, however, present variably.
In
fetal stage, ultrasound or fetal echocardiogram may reveal hydrocephalus,
and cardiac myoma.
At
birth, ash leaf spots and infantile spasms are characteristic.
In children, seizures predominate. The seizures are
mostly tonic-clonic or infantile myoclonic, though partial motor and complex partial seizures are also
seen. Petit mal attacks are lot common. The degree of mental retardation in these patients varies and regression has
been noticed in older patients. 45% of them may have normal intelligence.
Severely
affected children exhibit bizarre purposeless hand movements and posture,
but no true athetosis or chorea.
In later life, there
may be spastic hemiplegia or diplegia. They may
be due to either uncontrolled seizures or to the development of a brain
tumor. Motor deficits are rare, though they may be seen as a manifestation
of a brain tumor. There may be features of obstructive hydrocephalus, due
to intraventricular SEGA.
Roach et al has listed the following criteria for the diagnosis of TS.
|
Primary features
|
Secondary features.
|
Tertiary features.
|
|
Facial angiofibromas.
|
Affected 1st degree relative.
|
Hypomelonoic nodules.
|
|
Multiple ungual fibromas.
|
Cardiac rhabdomyoma (HPE/scan
+ve).
|
'Confetti" skin lesions.
|
|
Cortical tubers (HPE +ve).
|
Cortical tubers (CT+ve).
|
Renal cysts.
|
|
Subependymal nodules or
subependymal giant astrocstrocytoma (SEGA).
|
Noncalcified subependymal nodules
(CT+ve).
|
Enamel pits.
|
|
Multiple calcified subependymal nodules
protruding into ventricles (CT+ve).
|
Shagreen patches.
|
Hamartomatous rectal polyps
(HPE+ve).
|
|
Multiple retinal
hamartomas.
|
Forehead plaque.
|
Bone cyst (CT +ve).
|
|
|
Pulmonary Lymphangiomyomatosis
(HPE+ve).
|
Pulmonary lymphangiomyomatosis
(CT+ve).
|
|
|
Renal Angiomyolipoma (HPE+ve).
|
White matter heterotopias
(CT+ve).
|
|
|
Renal cysts (HPE+ve).
|
Hamartomas of other organs
(HPE+ve).
|
|
|
|
Infantile spasms.
|
Definite: one primary and
two sec or one sec and two tertiary;
Probable: one sec and one
tertiary or three tertiary;
Suspected: one sec or two
tertiary.
Imaging:
On CT,
cortical tubers, unless calcified, are difficult to
identify. The calcifications are mostly just
lateral to the foramen of Munro and in the body of the
lateral ventricle, though rarely, they may occur in
the wall of the third and fourth ventricles.The
tendency for these lesions to protrude into the lateral
ventricle, distinguishes them from other
calcified lesions seen in cytomegalovirus infection, cysticercosis
and toxoplasmosis. Other lesions which may encroach into the ventricles, e.g. heterotopic grey matter or
ependymomas are not multiply and do not calcify. Venticulomegaly, perhaps due to high CSF
protein may be seen in children.
MRI scan of the brain is the most sensitive study.
Cortical tubers appear as focally expanded gyri, which do not enhance. They are iso/hypodense intracerebral lesions are
seen especially in the frontal, parietal and occipital lobes, represent
areas of defective myelination and heterotopic hamartomatous tissue which
occur particularly at the junction of grey and white matter. These are seen
in 12-69% of cases, but are not diagnostic of TS when they occur in
isolation.
Bands of abnormal
signal intensity radiating from the ventricles to the cortical mantle and /
or wedge shaped lesions with their apex at the ventricle and their base at a cortical tuber. White matter
mass lesions appear less often; they are hyperdense on T2 and hypo/isodense
on T1.
Subependymal (SEGA) tumors are seen as isodense lesions enhancing
uniformly with contrast. They are located mainly
at the foramen of Munro and produce obstructive hydrocephalus. They may, occasionally, have a cystic component. Asymmetrical ventricular
dilatation may be seen in the
absence of tumor.
Management:
Treatment involves controlling seizures with antiepileptic drugs and special education for the mentally
handicapped.
ACTH ,
and lesionectomy is highly selected patients may help. The
life expectancy of these patients is decreased,
the causes of death being cardiac failure, brain tumors, status epilepticus and renal failure.
No need for surgical
intervention in asymptomatic patients. Asymptromatic children must be followed
up periodically.
The brain
tumors can be excised in adults with a good prognosis; subtotal
excision to relieve hydrocephalus,may suffice.
In children, the associated hydrocephalus
may be shunted, and the child is reviewed periodically.
Role of radiotherapy is controversial.
VON HIPPEL-LINDAU
DISEASE (retino
cerebellar angiomatosis):
The von
Hippel-Lindau (VHL) disease or complex is an autosomal
dominant disorder with variable expression, characterized
by either more than one hemangioblastoma
within the neuraxis associated with at
least one visceral manifestation. No cutaneous stigmata arc
seen in patients with VHL complex. It has an incidence of about one in
40,000 live births. It is probably caused by a gene complex that maps to
the short arm of chromosome 3.
The
association of retinal, cerebellar and visceral
lesions was made, in 1926. by Arvid Lindau, who started his work by
investigating cerebellar cysts. The retinal angiomas had been described earlier, by Collins, in
1894 and by von Hippel, in 1904. Brandt
published the autopsy results of von Hippel's patient and
described tumors in the viscera in addition to those
in the brain and the spinal cord.
Retinal angiomas arc seen in over 50 per
cent of patients with the VHL complex and may be the only finding in
children under 10 years of age. The lesions are seen mostly in the peripheral parts of the retina, though they
have also been recorded at the macula and the
optic disc. They are usually seen in both the eyes.. Photocoagulation is the
treatment of choice. As new lesions may appear in course of time, the
patients must be kept under regular ophthalmological
follow up.
|
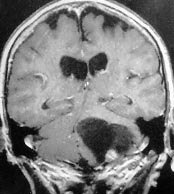
The typical lesion in
the neuraxis is a cerebellar hemangioblastoma, which at autopsy is found in at
least 60% of patients with the disease. Hemangioblastomas may also be found in the brain stem, spinal cord
and in the supratentorial compartment. The lesions may be solid or cystic.
They are commonly multiple, with the tumors appearing metachronously.
Angiomas may also be found in other
organs such as the liver, spleen, kidney, lung, the skeletal system,
epididymis, and the renal cortex.
However, the most common and dangerous tumors are
pheochromocytoma and renal cell carcinoma, which cause death in a significant proportion of VHL patients. Renal cell
carcinoma is seen in up to 25 per cent of patients with the VHL complex, and differs from its sporadic
counterpart in its earlier age of onset, multicentricity, and synchronous
or metachronous bilateral involvement.
|
|
|
|
Cystic
hemangioblastoma
-MRI
(cor)
|
|
NEUROCUTANEOUS
ANGIOMATOSES:
These are a group of genetic
disorders which have an abnormality of
blood vessels of the skin and nervous system as their only common feature, and arc grouped together for
convenience. Each syndrome has other systemic angiomata as well as
hematopoietic and immunological deficiencies.
Ataxia telangiectasia (Louis-Bar or Border-Sedgwick syndrome) is an autosomal recessive
disorder with progressive ataxia, cutaneous telangiectasias. Prognosis is
poor, with death usually occurring in the second decade due to infection or
neoplasia as a
|
result of
humoral and cellular immunodeficiency.
Sturge-Weber syndrome (Encephlotrigeminal angiomatosis) may be caused by a somatic
mutation occurring sporadically, rather than as an inherited disorder.
The characteristic skin lesion is a unilateral facial angioma (pot-wine
stain) in one or two dermatomes of the trigeminal nerve. There is an
ipsilateral parieto-occipital leptomeningeal venous angiomatosis with
underlying cortical atrophy. Calcification of the second and third
cortical layers of this region appear as ' rail road' calcification on
plain x-rays of the skull. Patient presents with seizures or hemiparesis.
SAH is rare.
In Klippel-Trennauney-Weber
syndrome (spinal cutaneous angiomatosis), the cutaneous angioma is
unilateral on the body, involving one or more
|
|

|
|
Port wine stain
|
|
dermatomes, with a
hemangioma of the spinal cord at the same level.
The lesion is seen as
a spinal variant of Sturge weber syndrome.
Fabry's disease (Angiokeratoma Corporis Diffusum) results from the accumulation of
ceramide trihexoside in the media and endothelium of small blood vessels,
due to a deficiency of alpha galactosidase. It is an X linked recessive
disorder, characterized by telangiectasias of the lower half of the body.
Skin lesions apart, renal function may be impaired with resultant hypertension
and myocardial infarction. More severe forms have diffuse involvement of
vessels of the peripheral nerves and of the CNS, leading to CVAs in young
adults. Painful polyneuropathy is another neurological problem.
Other rarer syndromes
include
Fibrous dysplasia (Albright's syndrome)-dysplasia of bones, irregular cafe-au-lait
pigmentation, sexual precocity in females, endocrine disturbances, mental
retardation, seizures and 'ground glass' radilogic appearance of bones.
Osler-weber-Rendu
syndrome (Hereditary hemorrhagic telengiectasia)-autosomal
dominant disease with angiomas of the skin, mucosal surfaces, and nervous
system, and usually presents with hemorrhage and should be excluded in all
patients with multiple AVMs, or family history of SAH, or repeated
epistaxis.
Wyburn-Mason syndrome -AVM in the midbrain with unilateral retinal and facial
malformations.
Neurocutaneous
melanosis (Rokitansky-van Bogaert syndrome)-cutaneous by
pigmented nevi, intracerebral melanotic pigmentations, and
hydrocephalus.
Incontinentia
pigmenti (Bloch-Sulzberger syndrome)-cutaneous bullae,
verrucation, crustation and pigmentations, and cerebral palsy and seizures.
Ocular, skeletal, and cerebral malformations may be there.
Multiple nevoid basal
cell carcinoma (Ward-Gorin-Goltz syndrome)-multiple basal cell
carcinomas. skeletal anomalies, congenital hydrocephalus,
medulloblastoma, visceral cysts and malformations.
Cutaneomeningospinal
angiomatosis (Berenbruch-Cushing-Cobb syndrome)-cutaneous vascular
nevus, angiomas in spinal cord, vertebrae and viscera.
Systemic angiomatosis (Ullmann's syndrome)-cavernous and telangiectatic angiomatosis of
CNS and viscera, cutaneous angioma.
Oculocerebral
angiomatosis (Bregeats's syndrome)-oculo-orbital angiomatosis,
thalamoencephalic angioma, cutaneous angioma.
Neurocutaneous
lipomatosis-intracranial and intraspinal lipomata,
leptomeningeal lipomatosis, facial; and axial cutaneous lipomata, visceral
lipomatosis, skull lipomatosis, cranial, cerebral, and spinal cord
anomalies.
|
